Brudno Jennifer N, Maus Marcela V, Hinrichs Christian S
Surgery Branch, Center for Cancer Research, National Cancer Institute, National Institutes of Health, Bethesda, Maryland.
Department of Medicine, Massachusetts General Hospital Cancer Center, Boston.
JAMA. 2024 Dec 10;332(22):1924-1935. doi: 10.1001/jama.2024.19462.
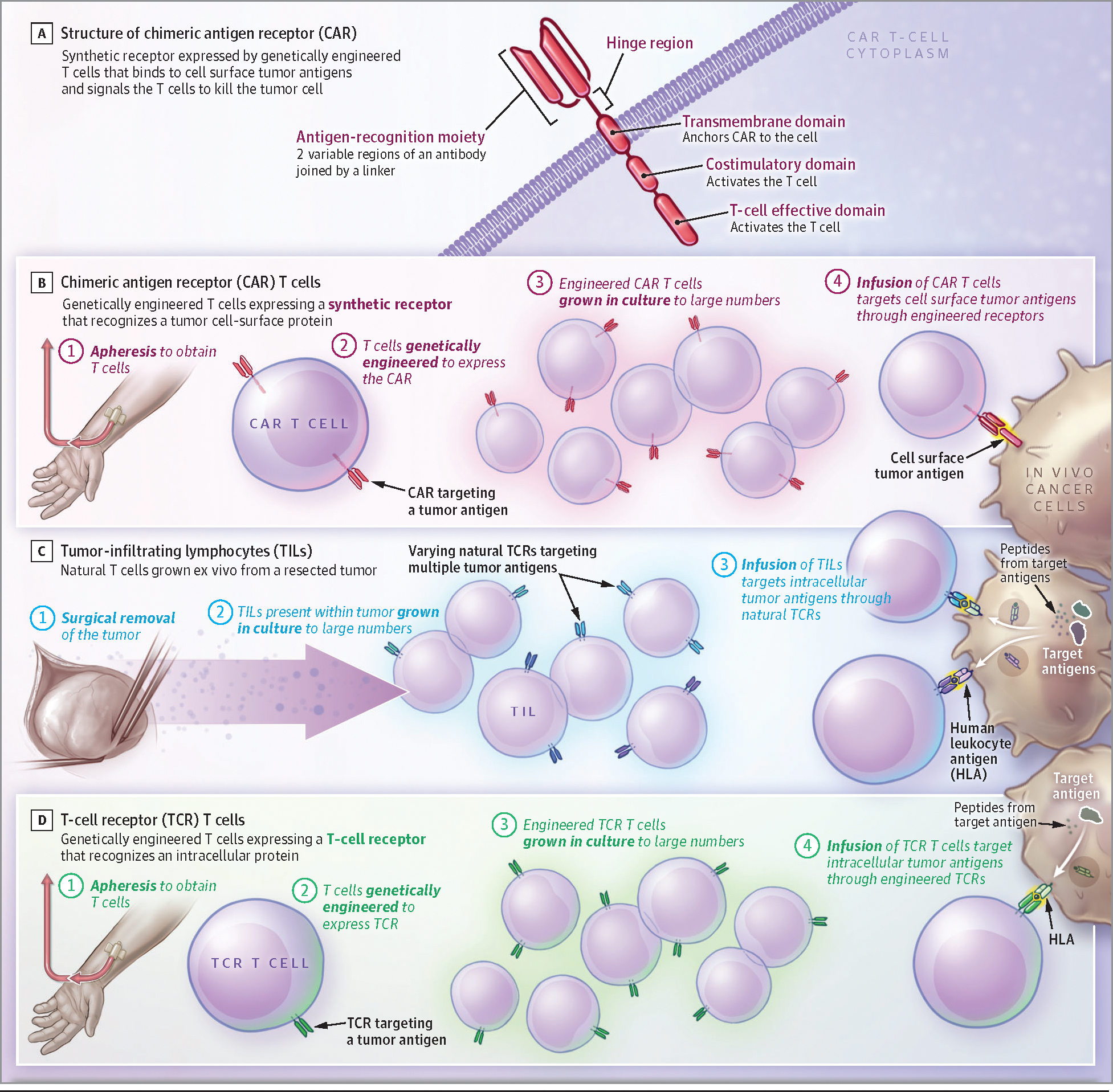
Chimeric antigen receptor (CAR) T cells are T lymphocytes that are genetically engineered to express a synthetic receptor that recognizes a tumor cell surface antigen and causes the T cell to kill the tumor cell. CAR T treatments improve overall survival for patients with large B-cell lymphoma and progression-free survival for patients with multiple myeloma.
Six CAR T-cell products are approved by the US Food and Drug Administration (FDA) for 6 hematologic malignancies: B-cell acute lymphoblastic leukemia, large B-cell lymphoma, follicular lymphoma, mantle cell lymphoma, chronic lymphocytic leukemia, and multiple myeloma. Compared with standard chemotherapy followed by stem cell transplant, CAR T cells improved 4-year overall survival in patients with large B-cell lymphoma (54.6% vs 46.0%). Patients with pediatric acute lymphoblastic leukemia achieved durable remission after CAR T-cell therapy. At 3-year follow-up, 48% of patients were alive and relapse free. In people with multiple myeloma treated previously with 1 to 4 types of non-CAR T-cell therapy, CAR T-cell therapy prolonged treatment-free remissions compared with standard treatments (in 1 trial, CAR T-cell therapy was associated with progression-free survival of 13.3 months compared with 4.4 months with standard therapy). CAR T-cell therapy is associated with reversible acute toxicities, such as cytokine release syndrome in approximately 40% to 95% of patients, and neurologic disorders in approximately 15% to 65%. New CAR T-cell therapies in development aim to increase efficacy, decrease adverse effects, and treat other types of cancer. No CAR T-cell therapies are FDA approved for solid tumors, but recently, 2 other T lymphocyte-based treatments gained approvals: 1 for melanoma and 1 for synovial cell sarcoma. Additional cellular therapies have attained responses for certain solid tumors, including pediatric neuroblastoma, synovial cell sarcoma, melanoma, and human papillomavirus-associated cancers. A common adverse effect occurring with these T lymphocyte-based therapies is capillary leak syndrome, which is characterized by fluid retention, pulmonary edema, and kidney dysfunction.
CAR T-cell therapy is an FDA-approved therapy that has improved progression-free survival for multiple myeloma, improved overall survival for large B-cell lymphoma, and attained high rates of cancer remission for other hematologic malignancies such as acute lymphoblastic leukemia, follicular lymphoma, and mantle cell lymphoma. Recently approved T lymphocyte-based therapies demonstrated the potential for improved outcomes in solid tumor malignancies.
嵌合抗原受体(CAR)T细胞是经过基因工程改造的T淋巴细胞,可表达一种识别肿瘤细胞表面抗原的合成受体,从而使T细胞杀死肿瘤细胞。CAR T细胞疗法可提高大B细胞淋巴瘤患者的总生存率,并提高多发性骨髓瘤患者的无进展生存率。
美国食品药品监督管理局(FDA)已批准6种CAR T细胞产品用于6种血液系统恶性肿瘤:B细胞急性淋巴细胞白血病、大B细胞淋巴瘤、滤泡性淋巴瘤、套细胞淋巴瘤、慢性淋巴细胞白血病和多发性骨髓瘤。与标准化疗后进行干细胞移植相比,CAR T细胞提高了大B细胞淋巴瘤患者的4年总生存率(54.6%对46.0%)。儿童急性淋巴细胞白血病患者在接受CAR T细胞治疗后实现了持久缓解。在3年的随访中,48%的患者存活且无复发。在先前接受过1至4种非CAR T细胞疗法治疗的多发性骨髓瘤患者中,与标准治疗相比,CAR T细胞疗法延长了无治疗缓解期(在1项试验中,CAR T细胞疗法的无进展生存期为13.3个月,而标准疗法为4.4个月)。CAR T细胞疗法与可逆的急性毒性相关,例如约40%至95%的患者出现细胞因子释放综合征,约15%至65%的患者出现神经系统疾病。正在研发的新型CAR T细胞疗法旨在提高疗效、减少不良反应并治疗其他类型的癌症。目前尚无FDA批准的用于实体瘤的CAR T细胞疗法,但最近,另外2种基于T淋巴细胞的疗法获得了批准:1种用于黑色素瘤,1种用于滑膜细胞肉瘤。其他细胞疗法在某些实体瘤中也取得了疗效,包括儿童神经母细胞瘤、滑膜细胞肉瘤、黑色素瘤和人乳头瘤病毒相关癌症。这些基于T淋巴细胞的疗法常见的不良反应是毛细血管渗漏综合征,其特征为液体潴留、肺水肿和肾功能障碍。
CAR T细胞疗法是一种经FDA批准的疗法,它提高了多发性骨髓瘤的无进展生存率,提高了大B细胞淋巴瘤的总生存率,并使其他血液系统恶性肿瘤(如急性淋巴细胞白血病、滤泡性淋巴瘤和套细胞淋巴瘤)获得了较高的癌症缓解率。最近批准的基于T淋巴细胞的疗法显示了在实体瘤恶性肿瘤中改善预后的潜力。