Research Center for Social Determinants of Health, Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran (the Islamic Republic of).
Social Development and Health Promotion Research Center, Health Institute, Kermanshah University of Medical Sciences, Kermanshah, Iran (the Islamic Republic of).
BMJ Open. 2024 Nov 4;14(11):e085035. doi: 10.1136/bmjopen-2024-085035.
This study represents a pioneering attempt to quantify the contribution of age, sex and socioeconomic status (SES) to the observed inequalities in lipid profile components.
Cross-sectional study.
The data from the Ravansar Non-Communicable Disease (RaNCD) Cohort Study were used.
10 000 individuals aged 35-65 years.
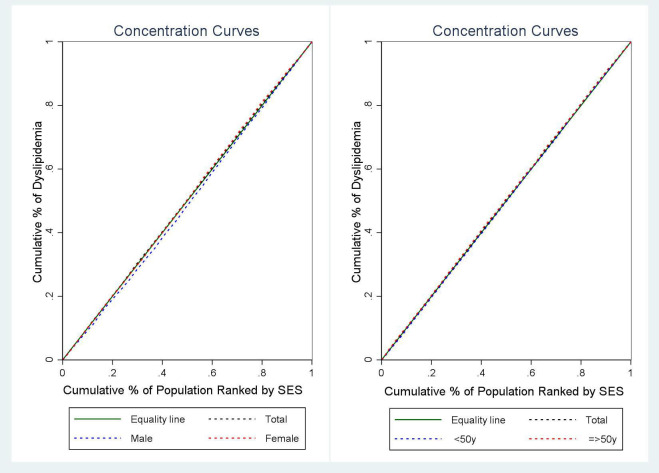
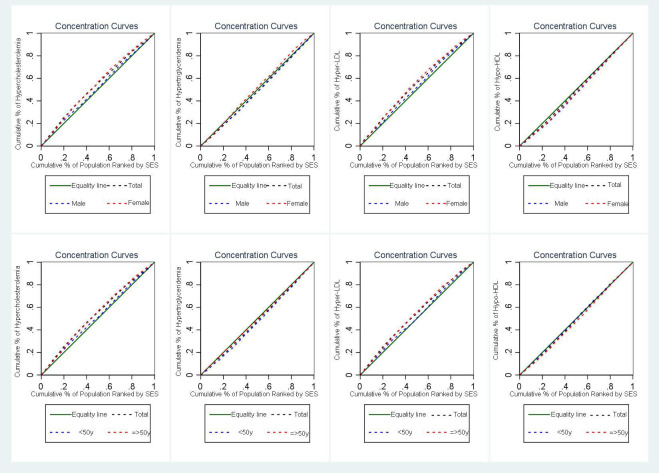
Principal component analysis was used to determine the SES of individuals. Using the concentration index (C-index) and curves, the study assessed socioeconomic inequalities in dyslipidaemia in different age groups and genders. Decomposition analysis was used to determine the contribution of sex, age and SES to the observed inequality in the prevalence of dyslipidaemia components between the wealthiest and poorest groups.
The prevalence of dyslipidaemia was 72.39% of the population and was significantly higher in women than in men (excluding hypertriglyceridaemia). Overall, no significant SES-based inequality in dyslipidaemia was observed (C-index=-0.045, p=0.116), but after adjustment for age and sex, individuals with high SES had increased odds of dyslipidaemia (OR=1.16, 95% CI: 1.03 to 1.31). Hypercholesterolaemia and hyper-low-density lipoprotein (LDL) were more common in individuals with lower SES (C-index=-0.117 and -0.105), while hypo-high-density lipoprotein (HDL) was more prevalent in individuals with higher SES (C-index=0.029), regardless of adjustment for age, sex and confounding factors. SES played a significant role in hypercholesterolaemia and hyper-LDL (322.11% and 400.14%), while sex dominated in hypertriglyceridaemia and hypo-HDL (814.05% and -615.26%) and contributed to the existing inequalities.
The results highlight the existing inequalities in lipid profiles due to SES, sex and age. Consideration of these factors in interventions and policy decisions is critical to reduce abnormalities and inform future interventions.
本研究旨在首次定量分析年龄、性别和社会经济地位(SES)对脂质谱成分观察到的不平等的贡献。
横断面研究。
使用拉万萨尔非传染性疾病(RaNCD)队列研究的数据。
10000 名年龄在 35-65 岁的个体。
使用主成分分析确定个体的 SES。使用集中指数(C 指数)和曲线评估不同年龄组和性别的血脂异常的社会经济不平等。分解分析用于确定性别、年龄和 SES 对最富有和最贫穷组之间观察到的血脂异常成分患病率的不平等的贡献。
血脂异常的患病率为人群的 72.39%,女性明显高于男性(不包括高甘油三酯血症)。总体而言,血脂异常不存在显著的 SES 相关不平等(C 指数=-0.045,p=0.116),但调整年龄和性别后,SES 较高的个体血脂异常的几率增加(OR=1.16,95%CI:1.03-1.31)。低 SES 个体更常见高胆固醇血症和低高密度脂蛋白(LDL)(C 指数=-0.117 和-0.105),而高 SES 个体更常见低高密度脂蛋白(HDL)(C 指数=0.029),无论是否调整年龄、性别和混杂因素。SES 在高胆固醇血症和高 LDL 血症中起重要作用(322.11%和 400.14%),而性别在高甘油三酯血症和低 HDL 血症中占主导地位(814.05%和-615.26%),并导致了现有的不平等。
结果突出了 SES、性别和年龄导致的脂质谱不平等。在干预措施和政策决策中考虑这些因素对于减少异常和为未来的干预措施提供信息至关重要。