Yadav Virendra Kumar, Mohan Suyash, Agarwal Sumeet, de Godoy Laiz Laura, Rajan Archith, Nasrallah MacLean P, Bagley Stephen J, Brem Steven, Loevner Laurie A, Poptani Harish, Singh Anup, Chawla Sanjeev
Centre for Biomedical Engineering, Indian Institute of Technology Delhi, New Delhi, India.
Department of Radiology, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA, USA.
Neurooncol Adv. 2024 Oct 3;6(1):vdae159. doi: 10.1093/noajnl/vdae159. eCollection 2024 Jan-Dec.
It is imperative to differentiate true progression (TP) from pseudoprogression (PsP) in glioblastomas (GBMs). We sought to investigate the potential of physiologically sensitive quantitative parameters derived from diffusion and perfusion magnetic resonance imaging (MRI), and molecular signature combined with machine learning in distinguishing TP from PsP in GBMs in the present study.
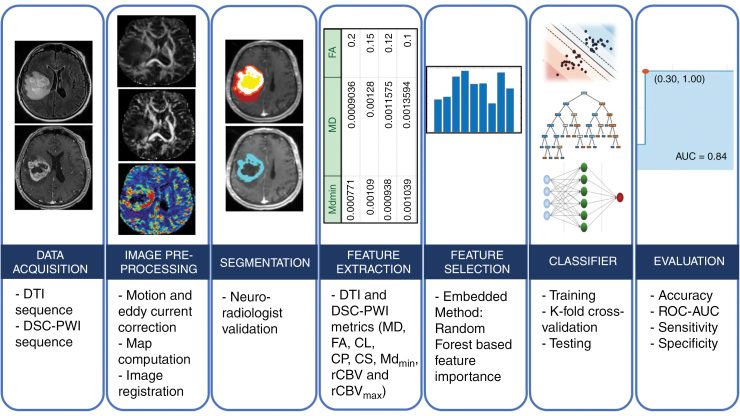
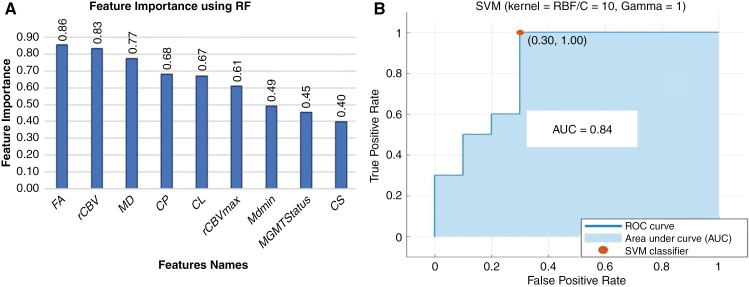
GBM patients ( = 93) exhibiting contrast-enhancing lesions within 6 months after completion of standard treatment underwent 3T MRI. Final data analyses were performed on 75 patients as O-methylguanine-DNA-methyltransferase (MGMT) status was available only from these patients. Subsequently, patients were classified as TP ( = 55) or PsP ( = 20) based on histological features or mRANO criteria. Quantitative parameters were computed from contrast-enhancing regions of neoplasms. PsP datasets were artificially augmented to achieve balanced class distribution in 2 groups (TP and PsP). A random forest algorithm was applied to select the optimized features. The data were randomly split into training and testing subsets in an 8:2 ratio. To develop a robust prediction model in distinguishing TP from PsP, several machine-learning classifiers were employed. The cross-validation and receiver operating characteristic (ROC) curve analyses were performed to determine the diagnostic performance.
The quadratic support vector machine was found to be the best classifier in distinguishing TP from PsP with a training accuracy of 91%, cross-validation accuracy of 86%, and testing accuracy of 85%. Additionally, ROC analysis revealed an accuracy of 85%, sensitivity of 70%, and specificity of 100%.
Machine learning using quantitative multiparametric MRI may be a promising approach to distinguishing TP from PsP in GBMs.
在胶质母细胞瘤(GBM)中,区分真正进展(TP)和假性进展(PsP)至关重要。在本研究中,我们试图探讨从扩散和灌注磁共振成像(MRI)得出的生理敏感定量参数以及分子特征结合机器学习在GBM中区分TP和PsP的潜力。
93例在完成标准治疗后6个月内出现强化病灶的GBM患者接受了3T MRI检查。由于仅从这75例患者中获得了O-甲基鸟嘌呤-DNA甲基转移酶(MGMT)状态,因此对这75例患者进行了最终数据分析。随后,根据组织学特征或mRANO标准将患者分为TP组(n = 55)或PsP组(n = 20)。从肿瘤的强化区域计算定量参数。对PsP数据集进行人工扩充,以实现两组(TP和PsP)的类分布平衡。应用随机森林算法选择优化特征。数据以8:2的比例随机分为训练子集和测试子集。为了建立一个强大的区分TP和PsP的预测模型,采用了几种机器学习分类器。进行交叉验证和受试者操作特征(ROC)曲线分析以确定诊断性能。
发现二次支持向量机是区分TP和PsP的最佳分类器,训练准确率为91%,交叉验证准确率为86%,测试准确率为85%。此外,ROC分析显示准确率为85%,敏感性为70%,特异性为100%。
使用定量多参数MRI的机器学习可能是区分GBM中TP和PsP的一种有前途的方法。