Stapleton Emma M, Metwali Nervana, Shlossman Michael, Wendt Linder, Pezzulo Alejandro A, Hamzeh Nabeel Y, Comellas Alejandro P, Thorne Peter S, Gerke Alicia K
University of Iowa.
Res Sq. 2024 Oct 22:rs.3.rs-5220174. doi: 10.21203/rs.3.rs-5220174/v1.
Sarcoidosis is a multi-system disease frequently affecting the lungs. It is thought to be mediated by gene-environment interaction; for example, epidemiological data show organic aerosol exposure increases risk of pulmonary sarcoidosis.
Does exposure to bioaerosol associate with worse lung disease in patients with pulmonary sarcoidosis?
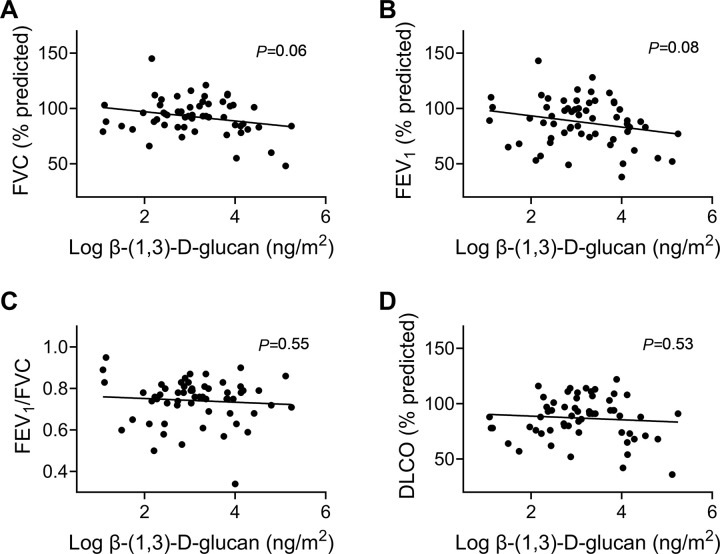
Using an observational, cohort study design, we measured residential exposure to fungal and bacterial cell wall material, β-(1,3)-D-glucan (BDG) and endotoxin, respectively, in healthy control subjects and those with pulmonary sarcoidosis. In the case cohort, we compared bioaerosol concentrations to pulmonary disease severity, assessed by pulmonary function testing, qualitative chest computed tomography (CT), and serum biomarkers. Log-transformed bioaerosol concentrations were compared to lung function and significance and correlation determined by Pearson correlation.
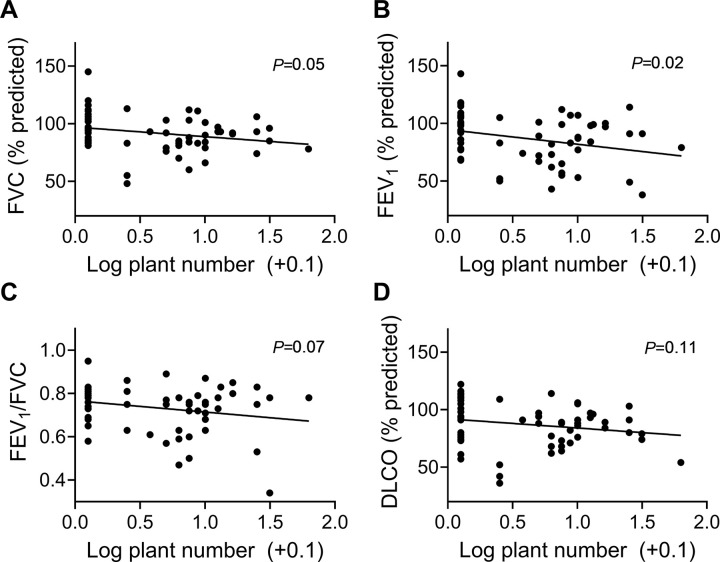
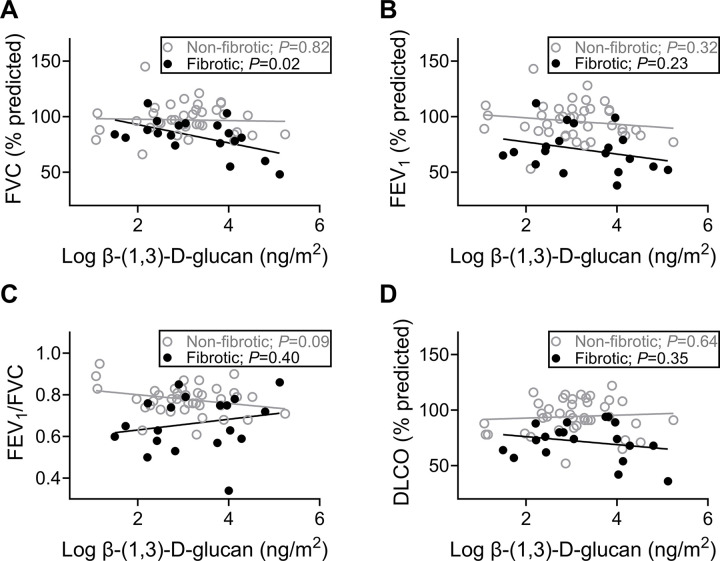
Homes of subjects with sarcoidosis had higher BDG and endotoxin concentrations than control subjects. Patients with significant pulmonary fibrosis had greater disease severity (Wasfi severity score, visual analogue scale) and reduced pulmonary function compared to those without fibrosis (all <0.01). Residential fungal BDG correlated with declining FVC, only in patients with fibrosis on CT imaging (=0.02). Survey data revealed higher BDG concentrations were found in homes of cat-owners, and the number of houseplants owned correlated with declines in FVC and FEV (=0.05 and 0.02, respectively). In patients without fibrosis, eight inflammatory markers correlated with BDG (6CKine/CCL21, IL-9, IL-17F, IL-21, IL-28A, I-309, MIP-1β, TARC), while in those with pulmonary fibrosis, BDG correlated with two inflammatory markers (Eotaxin-3, M-CSF), suggesting immune anergy to inhaled antigens in patients with fibrosis.
In patients with pulmonary fibrosis, disease severity was correlated with residential exposure to fungal cell wall material, but not gram-negative bacterial cell wall material. These patients may experience immune anergy to inhaled antigens.
结节病是一种常累及肺部的多系统疾病。其发病被认为是基因与环境相互作用介导的;例如,流行病学数据显示接触有机气溶胶会增加患肺结节病的风险。
肺结节病患者接触生物气溶胶是否与更严重的肺部疾病相关?
采用观察性队列研究设计,我们分别测量了健康对照者和肺结节病患者家庭环境中真菌和细菌细胞壁物质β-(1,3)-D-葡聚糖(BDG)和内毒素的暴露情况。在病例队列中,我们将生物气溶胶浓度与通过肺功能测试、定性胸部计算机断层扫描(CT)和血清生物标志物评估的肺部疾病严重程度进行比较。对生物气溶胶浓度进行对数转换后与肺功能进行比较,并通过Pearson相关性确定其显著性和相关性。
结节病患者家庭中的BDG和内毒素浓度高于对照者。与无纤维化患者相比,有显著肺纤维化的患者疾病严重程度更高(Wasfi严重程度评分,视觉模拟量表)且肺功能下降(均<0.01)。仅在CT成像显示有纤维化的患者中,家庭环境中的真菌BDG与用力肺活量(FVC)下降相关(=0.02)。调查数据显示,养猫家庭中的BDG浓度较高,所拥有的室内植物数量与FVC和第一秒用力呼气容积(FEV)下降相关(分别为=0.05和0.02)。在无纤维化的患者中,八种炎症标志物与BDG相关(6CKine/CCL21、白细胞介素-9、白细胞介素-17F、白细胞介素-21、白细胞介素-28A、I-309、巨噬细胞炎性蛋白-1β、胸腺活化调节趋化因子),而在有肺纤维化的患者中,BDG与两种炎症标志物相关(嗜酸性粒细胞趋化因子-3、巨噬细胞集落刺激因子),这表明纤维化患者对吸入抗原存在免疫无反应性。
在肺纤维化患者中,疾病严重程度与家庭环境中真菌细胞壁物质的暴露相关,但与革兰氏阴性细菌细胞壁物质无关。这些患者可能对吸入抗原存在免疫无反应性。