Department of Family and Community Medicine, University of California, Davis, Sacramento.
The Center for Healthcare Policy and Research, University of California, Davis, Sacramento.
JAMA Netw Open. 2024 Nov 4;7(11):e2441826. doi: 10.1001/jamanetworkopen.2024.41826.
Acute back pain is a common reason for primary care visits and often results in low-value spinal imaging.
To evaluate the effect of a standardized patient-delivered intervention on rates of low-value spinal imaging among primary care patients with acute low back pain.
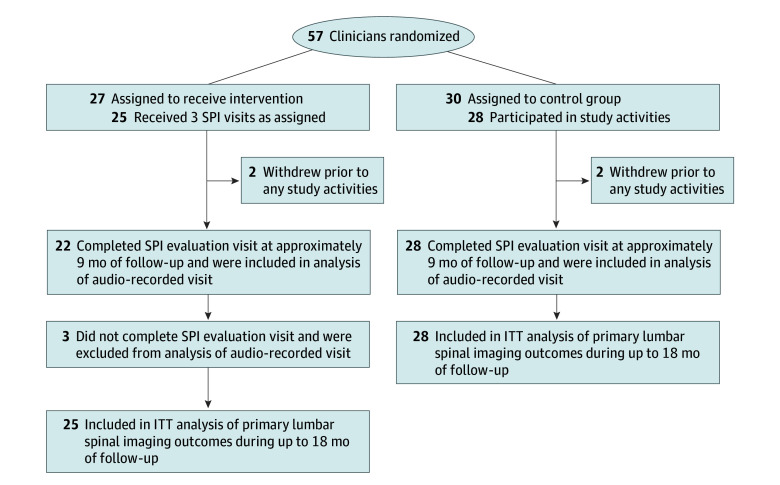
DESIGN, SETTING, AND PARTICIPANTS: In this randomized clinical trial, physicians or advanced practice clinicians were recruited from March 22 to August 5, 2021, from 10 adult primary care or urgent care clinics in Sacramento, California. The intervention period was from May 1, 2021, to March 30, 2022, with follow-up from October 28, 2021, to June 30, 2023. Analyses were performed from April 1 to June 25, 2024.
Clinicians were randomized 1:1 to intervention or control. Intervention clinicians received 3 simulated office visits, each with a standardized patient instructor (SPI) portraying a patient with acute uncomplicated back pain. At each visit, SPIs provided clinician feedback guided by a 3-step model: (1) set the stage for deferred imaging by building trust, (2) convey empathy, and (3) communicate optimism while advocating watchful waiting without imaging. Control clinicians received no intervention.
The primary outcome was lumbar spinal imaging completion within 90 days of acute low back pain visits, with study clinicians assessed up to 18 months of follow-up. Secondary outcomes were cervical spine imaging completion after acute neck pain visits, any imaging completion after an adult visit, patient experience ratings of clinicians (scale range, 0-100), and use of targeted communication skills during an audio-recorded standardized patient evaluation visit at median follow-up of 16.8 months (range, 14.1-18.0 months).
The analysis included 53 clinicians; mean (SD) age was 46.7 (1.0) years, and 35 (66.0%) reported female gender. A total of 25 were in the intervention group and 28 in the control group. After adjustment for prerandomization rates, patients with acute low back pain who saw intervention and control clinicians during follow-up had similar rates of lumbar imaging (194 of 1234 clinic visits [15.7%] vs 226 of 1306 clinic visits [17.3%]; adjusted ratio of postintervention vs preintervention odds ratios [AORR], 1.00; 95% CI, 0.72-1.40). Adjusted follow-up rates of imaging for acute neck pain (AORR, 1.16; 95% CI, 0.83-1.63) and overall imaging (AORR, 1.07; 95% CI, 0.97-1.19) were not significantly different among patients of intervention and control clinicians. Intervention and control clinicians had similar mean (SD) patient experience ratings during follow-up (88.6 [28.7] vs 88.8 [28.3]; adjusted mean difference-in-differences, -1.0; 95% CI, -3.0 to 0.9). During audio-recorded standardized patient visits, intervention clinicians had significantly better ratings than controls on eliciting the patient's perspective (adjusted standardized difference [ASD], 0.62; 95% CI, 0.05-1.19) and conveying empathy (ASD, 1.16; 95% CI, 0.55-1.77).
In this randomized clinical trial of an educational intervention using simulated office visits to encourage a watchful waiting approach for acute low back pain, the intervention had no significant effect on low-value spinal imaging rates or patient experience ratings.
ClinicalTrials.gov Identifier: NCT04255199.
急性背痛是初级保健就诊的常见原因,通常导致低价值的脊柱成像。
评估标准化患者提供的干预措施对初级保健急性腰痛患者低价值脊柱成像率的影响。
设计、地点和参与者:在这项随机临床试验中,从 2021 年 3 月 22 日至 8 月 5 日,从加利福尼亚州萨克拉门托的 10 个成人初级保健或紧急护理诊所招募医生或高级执业临床医生。干预期为 2021 年 5 月 1 日至 2022 年 3 月 30 日,随访时间为 2023 年 10 月 28 日至 6 月 30 日。分析于 2024 年 4 月 1 日至 6 月 25 日进行。
临床医生以 1:1 的比例随机分为干预组或对照组。干预组临床医生接受了 3 次模拟办公室就诊,每次都有一名标准化患者指导员(SPI)扮演急性单纯性背痛的患者。在每次就诊中,SPI 都根据一个三步模型为临床医生提供反馈:(1)通过建立信任来为推迟成像做好准备,(2)表达同理心,(3)在不进行成像的情况下提倡观察等待时传递乐观情绪。对照组临床医生未接受干预。
主要结果是急性腰痛就诊后 90 天内完成腰椎成像,研究临床医生在 18 个月的随访中进行评估。次要结果是急性颈痛就诊后完成颈椎成像、成人就诊后完成任何成像、患者对临床医生的体验评分(范围为 0-100),以及在中位随访 16.8 个月(范围为 14.1-18.0 个月)时对音频记录的标准化患者评估就诊时使用的靶向沟通技巧。
分析包括 53 名临床医生;平均(SD)年龄为 46.7(1.0)岁,35 名(66.0%)报告为女性。共有 25 名在干预组,28 名在对照组。在调整预随机率后,在随访期间接受干预和对照临床医生治疗的急性腰痛患者的腰椎成像率相似(1234 次就诊中有 194 次[15.7%],1306 次就诊中有 226 次[17.3%];调整后干预与预干预比值比[AORR],1.00;95%置信区间[CI],0.72-1.40)。急性颈痛(AORR,1.16;95%CI,0.83-1.63)和整体成像(AORR,1.07;95%CI,0.97-1.19)的调整随访率在干预和对照临床医生的患者中没有显著差异。干预和对照临床医生在随访期间的患者体验评分相似(88.6[28.7]与 88.8[28.3];调整后的差异-差异平均值,-1.0;95%CI,-3.0 至 0.9)。在音频记录的标准化患者就诊中,干预组临床医生在引出患者观点(调整后的标准化差异[ASD],0.62;95%CI,0.05-1.19)和表达同理心(ASD,1.16;95%CI,0.55-1.77)方面的评分明显优于对照组。
在这项使用模拟就诊鼓励急性腰痛观察等待方法的教育干预随机临床试验中,该干预措施对低价值脊柱成像率或患者体验评分没有显著影响。
ClinicalTrials.gov 标识符:NCT04255199。