Mahmoudjafari Zahra, Bhatt Valkal, Galvin John, Xue Zhenyi, Zeiser Robert, Locatelli Franco, Socié Gérard, Mohty Mohamad
University of Kansas Cancer Center, Westwood, KS, USA.
Incyte Corporation, Wilmington, DE, USA.
Bone Marrow Transplant. 2025 Jan;60(1):69-78. doi: 10.1038/s41409-024-02445-6. Epub 2024 Nov 6.
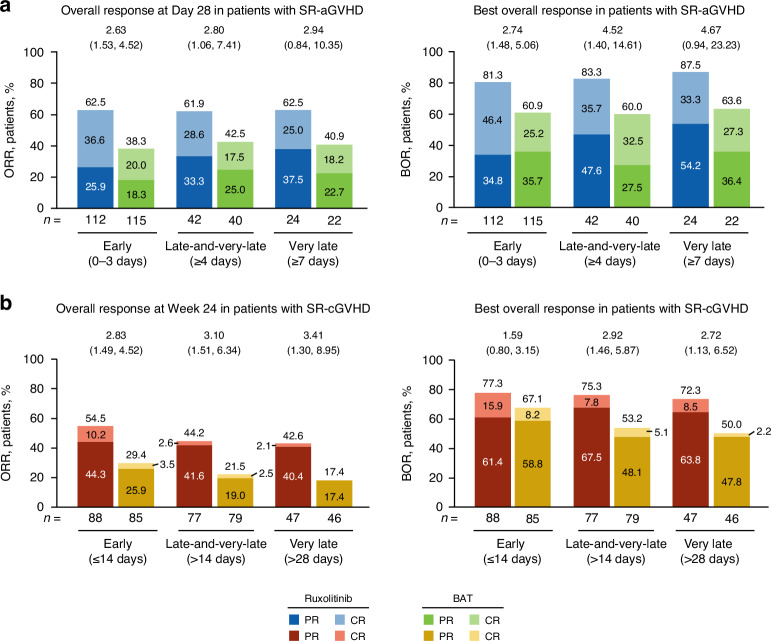
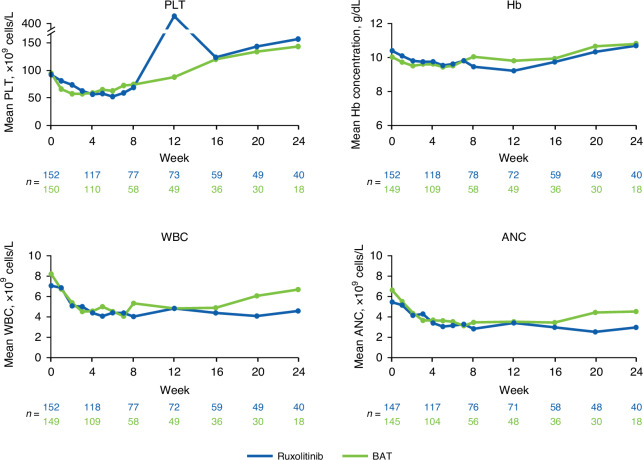
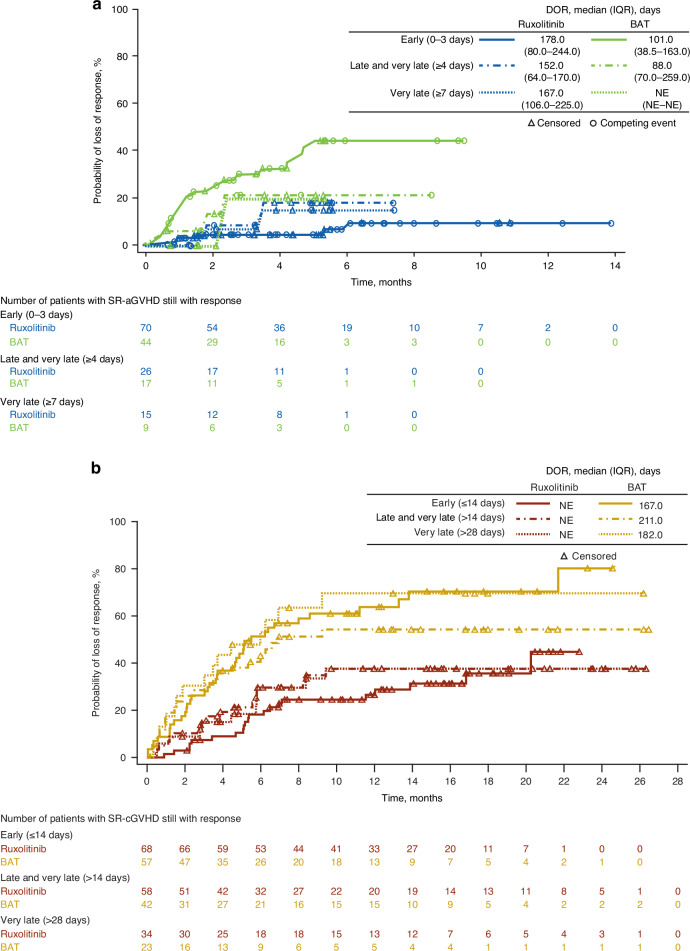
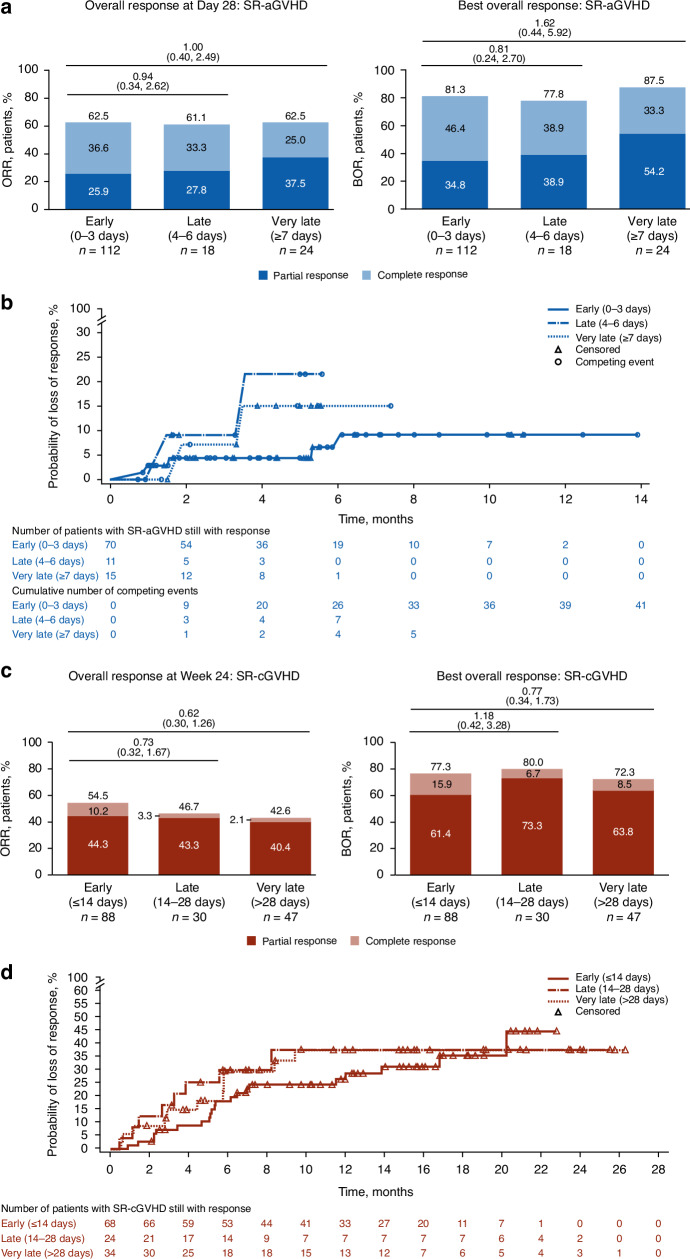
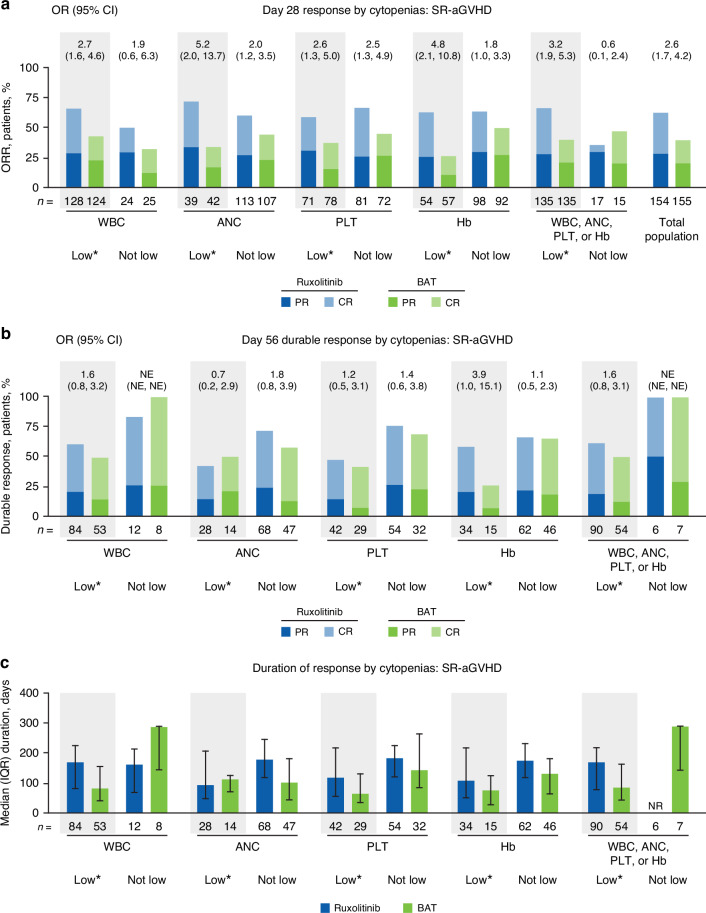
REACH2 and REACH3 were randomized, multicenter, open-label phase 3 studies comparing the selective Janus kinase (JAK)1/JAK2 inhibitor ruxolitinib versus investigators' choice of best available therapy (BAT) in steroid-refractory (SR) acute (REACH2) or chronic (REACH3) graft-versus-host disease (aGVHD/cGVHD). Moderate-severe aGVHD/cGVHD can progress rapidly; thus, key clinical considerations driving management of patients with SR-aGVHD/SR-cGVHD are prompt treatment initiation and concomitant cytopenias. These post hoc analyses of REACH2/REACH3 describe the impact of timing of treatment initiation after SR-aGVHD/SR-cGVHD diagnosis and development of concomitant cytopenias on treatment outcomes. Ruxolitinib initiation within 3 days from SR-aGVHD diagnosis yielded an extended duration of response and higher Day 28 complete response rates compared with initiation ≥7 days after SR-aGVHD diagnosis (median 178 vs 167 days and 36.6% vs 25.0%, respectively). For patients with SR-cGVHD, Week 24 overall response was not impacted by time to treatment (54.5% vs 42.6% for <14 vs >28 days). Clinically relevant cytopenias were manageable, allowing for maintenance of dose intensity (median 20 mg/d), and did not impact the favorable efficacy outcomes from ruxolitinib treatment. This analysis highlights the practical importance of considering earlier ruxolitinib initiation after SR diagnosis in GVHD and the benefits of ruxolitinib treatment compared with BAT even for patients with cytopenias.
REACH2和REACH3是随机、多中心、开放标签的3期研究,比较选择性Janus激酶(JAK)1/JAK2抑制剂芦可替尼与研究者选择的最佳可用疗法(BAT)用于治疗类固醇难治性(SR)急性(REACH2)或慢性(REACH3)移植物抗宿主病(aGVHD/cGVHD)。中重度aGVHD/cGVHD可迅速进展;因此,推动SR-aGVHD/SR-cGVHD患者管理的关键临床考虑因素是及时开始治疗和并发血细胞减少。这些对REACH2/REACH3的事后分析描述了SR-aGVHD/SR-cGVHD诊断后开始治疗的时间以及并发血细胞减少的发生对治疗结果的影响。与SR-aGVHD诊断后≥7天开始治疗相比,在SR-aGVHD诊断后3天内开始使用芦可替尼可延长缓解持续时间并提高第28天的完全缓解率(分别为中位数178天对167天以及36.6%对25.0%)。对于SR-cGVHD患者,第24周的总体缓解率不受治疗时间的影响(诊断后<14天与>28天开始治疗的患者分别为54.5%对42.6%)。临床相关的血细胞减少是可控的,可维持剂量强度(中位数20mg/d),并且不影响芦可替尼治疗的良好疗效结果。该分析强调了在GVHD中SR诊断后尽早开始使用芦可替尼的实际重要性,以及与BAT相比芦可替尼治疗的益处,即使对于有血细胞减少的患者也是如此。