MRC Clinical Trials Unit at University College London, Aviation House, 125 Kingsway, London, WC28 6NH, UK.
Mbale Clinical Research Institute, Pallisa Road, Mbale, PO Box 291, Uganda.
BMC Med. 2024 Nov 6;22(1):516. doi: 10.1186/s12916-024-03712-5.
African children with severe malaria are at increased risk of non-typhoidal salmonellae co-infection. Broad-spectrum antibiotics are recommended by guidelines but the optimal class and dose have not been established. We investigated the optimal dose of oral dispersible azithromycin and whether simple clinical criteria and point-of-care biomarkers could target antibiotics to those at greatest risk of bacterial co-infection.
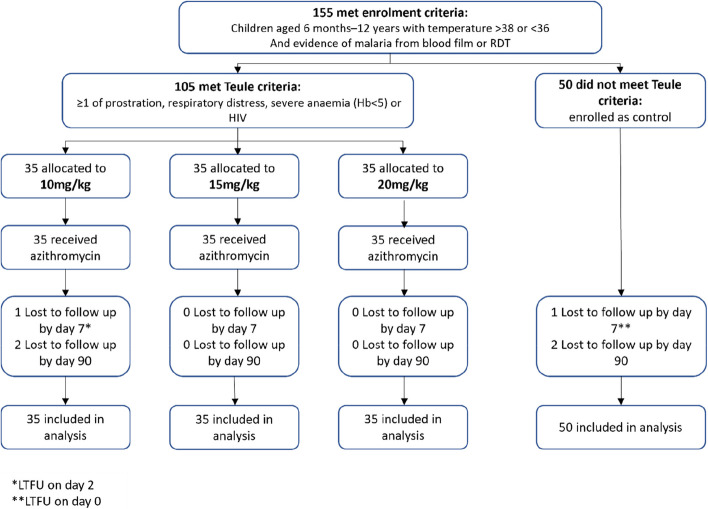
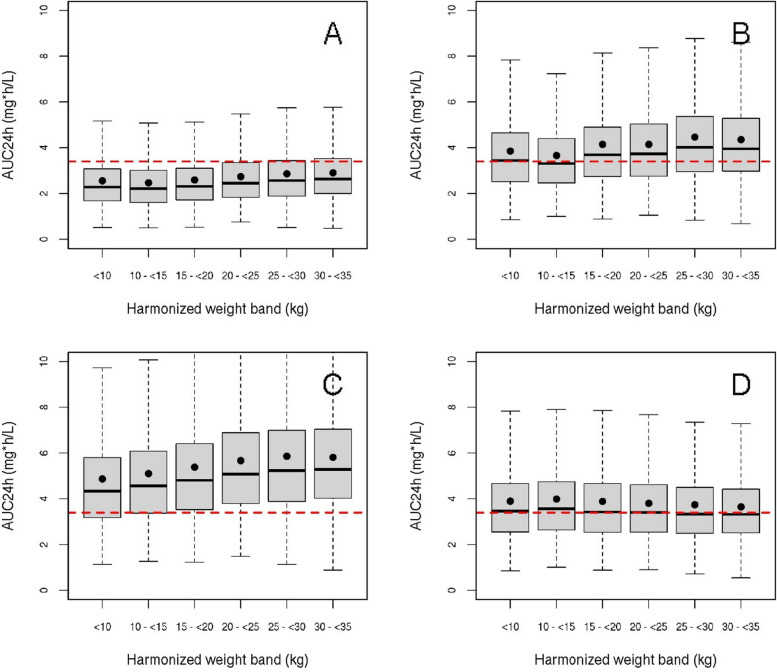
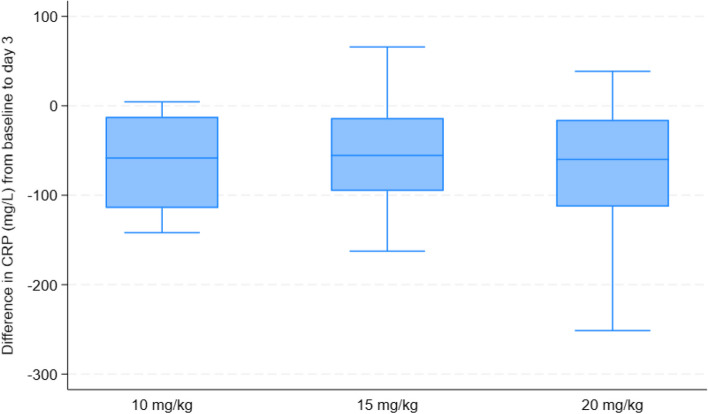
We conducted a phase I/II trial in Ugandan children with severe malaria comparing a 5-day course of azithromycin: 10, 15 and 20 mg/kg of azithromycin (prescribed by weight bands) spanning the dose-range effective for other salmonellae infection. We generated relevant pharmacokinetic (PK) data by sparse sampling during dosing intervals and investigated associations between azithromycin exposure and potential mechanisms (PK-pharmacodynamics) using change in C-reactive protein (CRP), a putative marker of sepsis, at 72 h (continuous) and microbiological cure (7-day) (binary), alone and as a composite with 7-day and 90-day survival. To assess whether clinical or biomarkers could identify those at risk of sepsis, a non-severe malaria control was concurrently enrolled.
Between January 2020 and January 2022, 105 cases were randomised azithromycin doses: 35 to 10 mg/kg, 35 to 15 mg/kg and 35 to 20 mg/kg. Fifty non-severe malaria controls were concurrently enrolled. CRP reduced in all arms by 72 h with a mean reduction of 65.8 mg/L (95% CI 57.1, 74.5) in the 10 mg/kg arm, 64.8 mg/L (95% CI 56.5, 73.1; p = 0.87) in the 20 mg/kg arm and a smaller reduction 51.2 mg/L (95% CI 42.9, 59.5; p = 0.02) in the 15 mg/kg arm. Microbiological cure alone outcome was not analysed as only one pathogen was found among cases. Three events contributed to the composite outcome of 7-day survival and microbiological cure, with no events in the 15 mg/kg arm. The odds ratio comparing 20 vs 10 mg/kg was 0.50 (95% CI 0.04, 5.79); p = 0.58. Due to the low number of pathogens identified, it was not possible to identify better methods for targeting antibiotics including both the cases and controls.
We found no evidence for an association between systemic azithromycin exposure and reduction in CRP. Further work is needed to better identify children at highest risk from bacterial co-infection.
ISRCTN49726849 (registered on 27th October 2017).
患有重症疟疾的非洲儿童存在感染非伤寒沙门氏菌的风险增加。指南推荐使用广谱抗生素,但尚未确定最佳类别和剂量。我们研究了口服分散片阿奇霉素的最佳剂量,以及简单的临床标准和即时检测生物标志物是否可以将抗生素靶向用于那些最有可能发生细菌合并感染的患者。
我们在乌干达的重症疟疾儿童中进行了一项 I/II 期试验,比较了 5 天疗程的阿奇霉素:10、15 和 20mg/kg 的阿奇霉素(按体重带划分剂量),涵盖了对其他沙门氏菌感染有效的剂量范围。我们通过在给药间隔期间进行稀疏采样生成了相关的药代动力学(PK)数据,并通过在第 72 小时(连续)和微生物学治愈(第 7 天)(二分类)时 C 反应蛋白(CRP)的变化(分类),单独和作为复合指标与第 7 天和 90 天生存率来研究阿奇霉素暴露与潜在机制(PK-药效学)之间的关系。为了评估临床或生物标志物是否可以识别出有发生败血症风险的患者,同时还纳入了非重症疟疾对照组。
2020 年 1 月至 2022 年 1 月期间,共随机分配了 105 例重症疟疾患者接受阿奇霉素剂量:35 例至 10mg/kg、35 例至 15mg/kg 和 35 例至 20mg/kg。同时纳入了 50 例非重症疟疾对照组。所有组的 CRP 在第 72 小时均有下降,其中 10mg/kg 组平均下降 65.8mg/L(95%CI 57.1,74.5),20mg/kg 组下降 64.8mg/L(95%CI 56.5,73.1;p=0.87),15mg/kg 组下降幅度较小,为 51.2mg/L(95%CI 42.9,59.5;p=0.02)。由于仅在病例中发现了一种病原体,因此未对微生物学治愈的单独结果进行分析。三个事件导致 7 天生存率和微生物学治愈的复合结果,而在 15mg/kg 组没有发生事件。20mg/kg 与 10mg/kg 比较的优势比为 0.50(95%CI 0.04,5.79);p=0.58。由于确定的病原体数量较少,因此无法确定针对包括病例和对照组在内的抗生素的更好方法。
我们没有发现全身阿奇霉素暴露与 CRP 降低之间存在关联的证据。需要进一步的工作来更好地识别出最有可能发生细菌合并感染的儿童。
ISRCTN49726849(于 2017 年 10 月 27 日注册)。