Infectious Disease Epidemiology Department, London School of Hygiene & Tropical Medicine, London, UK.
Infectious Disease Epidemiology Department, London School of Hygiene & Tropical Medicine, London, UK.
Lancet Infect Dis. 2023 Nov;23(11):1280-1290. doi: 10.1016/S1473-3099(23)00233-5. Epub 2023 Jul 13.
Bacteria of the order Enterobacterales are common pathogens causing bloodstream infections in sub-Saharan Africa and are frequently resistant to third-generation cephalosporin antibiotics. Although third-generation cephalosporin resistance is believed to lead to adverse outcomes, this relationship is difficult to quantify and has rarely been studied in this region. We aimed to measure the effects associated with resistance to third-generation cephalosporins in hospitalised patients with Enterobacterales bloodstream infection in Africa.
We conducted a prospective, matched, parallel cohort study at eight hospitals across sub-Saharan Africa. We recruited consecutive patients of all age groups with laboratory-confirmed Enterobacterales bloodstream infection and matched them to at least one patient without bloodstream infection on the basis of age group, hospital ward, and admission date. Date of infection onset (and enrolment) was defined as the day of blood sample collection for culturing. Patients infected with bacteria with a cefotaxime minimum inhibitory concentration of 1 mg/L or lower were included in the third-generation cephalosporin-susceptible (3GC-S) cohort, and the remainder were included in the third-generation cephalosporin-resistant (3GC-R) cohort. The primary outcomes were in-hospital death and death within 30 days of enrolment. We used adjusted multivariable regression models to first compare patients with bloodstream infection against matched patients within the 3GC-S and 3GC-R cohorts, then compared estimates between cohorts.
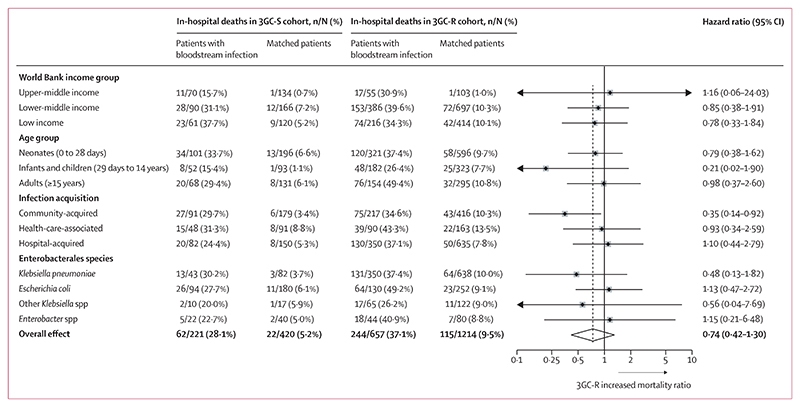
Between Nov 1, 2020, and Jan 31, 2022, we recruited 878 patients with Enterobacterales bloodstream infection (221 [25·2%] to the 3GC-S cohort and 657 [74·8%] to the 3GC-R cohort) and 1634 matched patients (420 [25·7%] and 1214 [74·3%], respectively). 502 (57·2%) bloodstream infections occurred in neonates and infants (age 0-364 days). Klebsiella pneumoniae (393 [44·8%] infections) and Escherichia coli (224 [25·5%] infections) were the most common Enterobacterales species identified. The proportion of patients who died in hospital was higher in patients with bloodstream infection than in matched controls in the 3GC-S cohort (62 [28·1%] of 221 vs 22 [5·2%] of 420; cause-specific hazard ratio 6·79 [95% CI 4·06-11·37] from Cox model) and the 3GC-R cohort (244 [37·1%] of 657 vs 115 [9·5%] of 1214; 5·01 [3·96-6·32]). The ratio of these cause-specific hazard ratios showed no significant difference in risk of in-hospital death in the 3GC-R cohort versus the 3GC-S cohort (0·74 [0·42-1·30]). The ratio of relative risk of death within 30 days (0·82 [95% CI 0·53-1·27]) also indicated no difference between the cohorts.
Patients with bloodstream infections with Enterobacterales bacteria either resistant or susceptible to third-generation cephalosporins had increased mortality compared with uninfected matched patients, with no differential effect related to third-generation cephalosporin-resistance status. However, this finding does not account for time to appropriate antibiotic treatment, which remains clinically important to optimise. Measures to prevent transmission of Enterobacterales could reduce bloodstream infection-associated mortality from both drug-resistant and drug-susceptible bacterial strains in Africa.
Bill & Melinda Gates Foundation.
肠杆菌目细菌是撒哈拉以南非洲地区血流感染的常见病原体,且常对第三代头孢菌素抗生素耐药。虽然第三代头孢菌素耐药被认为会导致不良后果,但在该地区,这种关系很难量化,也很少有研究。我们旨在衡量非洲肠杆菌目血流感染患者对第三代头孢菌素耐药的相关影响。
我们在撒哈拉以南非洲的 8 家医院进行了一项前瞻性、匹配、平行队列研究。我们招募了所有年龄组的实验室确诊的肠杆菌目血流感染患者,并根据年龄组、医院病房和入院日期与至少一名无血流感染的患者进行匹配。感染发病日期(和入组日期)定义为采集培养血样的日期。将头孢噻肟最低抑菌浓度为 1mg/L 或更低的细菌感染患者纳入第三代头孢菌素敏感(3GC-S)组,其余患者纳入第三代头孢菌素耐药(3GC-R)组。主要结局是院内死亡和入组后 30 天内死亡。我们使用调整后的多变量回归模型,首先比较 3GC-S 组和 3GC-R 组的血流感染患者与匹配患者,然后比较两组之间的估计值。
2020 年 11 月 1 日至 2022 年 1 月 31 日,我们招募了 878 名肠杆菌目血流感染患者(3GC-S 组 221 例[25.2%],3GC-R 组 657 例[74.8%])和 1634 名匹配患者(3GC-S 组 420 例[25.7%],3GC-R 组 1214 例[74.3%])。502 例(57.2%)血流感染发生在新生儿和婴儿(0-364 天)。最常见的肠杆菌目物种是肺炎克雷伯菌(393 例[44.8%]感染)和大肠杆菌(224 例[25.5%]感染)。与匹配对照组相比,3GC-S 组(221 例中的 62 例[28.1%] vs. 420 例中的 22 例[5.2%];Cox 模型中的病因特异性危险比 6.79[95%CI 4.06-11.37])和 3GC-R 组(657 例中的 244 例[37.1%] vs. 1214 例中的 115 例[9.5%];5.01[3.96-6.32])的血流感染患者的院内死亡率更高。3GC-R 组与 3GC-S 组的病因特异性危险比的比值(0.74[0.42-1.30])表明,在院内死亡风险方面没有显著差异。30 天内相对死亡风险的比值(0.82[95%CI 0.53-1.27])也表明两组之间没有差异。
无论是对第三代头孢菌素耐药还是敏感的肠杆菌目血流感染患者,与未感染的匹配患者相比,死亡率均增加,与第三代头孢菌素耐药状态无关。然而,这一发现并未考虑到及时给予适当抗生素治疗的情况,这在临床上对于优化治疗仍然很重要。预防肠杆菌目传播的措施可以降低非洲地区耐药和敏感细菌株血流感染相关的死亡率。
比尔及梅琳达·盖茨基金会。