Singh Abhishek, Hussain M A, Chaudhary Shyam Chand, Bharadwaj Akriti, Sawalani K K, Pradhan Akshyaya, Sethi Rishi
Department of Cardiology, King George's Medical University, Lucknow 226003, India.
Department of Internal Medicine, King George's Medical University, Lucknow 226003, India.
Cardiol Res Pract. 2024 Oct 30;2024:1489008. doi: 10.1155/2024/1489008. eCollection 2024.
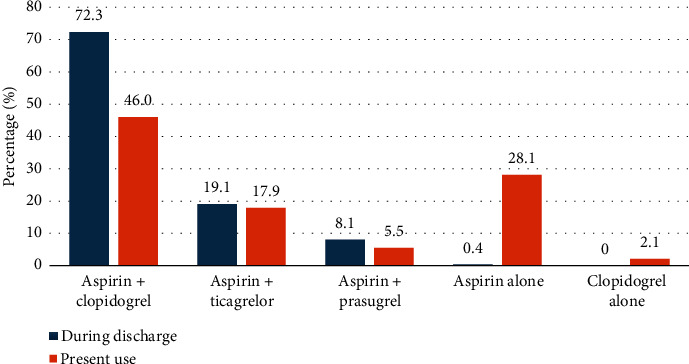
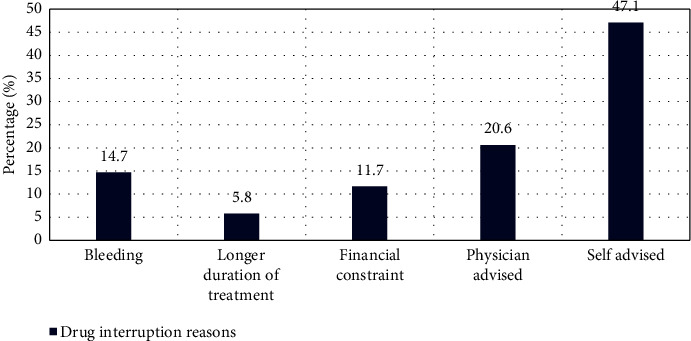
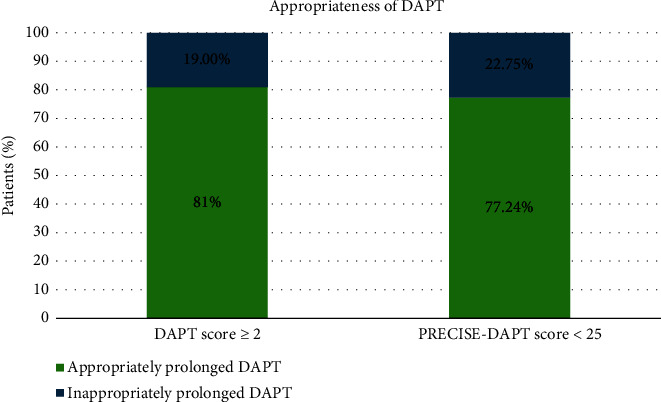
Utilizing the two available prediction models, i.e., the dual antiplatelet therapy (DAPT) score and predicting bleeding complication in patients undergoing stent implantation and subsequent dual antiplatelet therapy (PRECISE-DAPT) score, we aimed to determine the appropriateness of the DAPT in patients with acute myocardial infarction (AMI) in patients undergoing percutaneous coronary intervention (PCI). We retrospectively enrolled 235 patients of AMI and for all the patients and thorough information regarding history, risk factors, and medications were collected. Both DAPT and PRECISE-DAPT scores were calculated. The patients were divided by their recommended cutoffs and the appropriateness of the duration of the recommended DAPT was measured based on the observed scores. Bleeding academic research consortium (BARC) classification was used to define the bleeding events. In the patients with DAPT score ≥ 2 and PRESICE-DAPT < 25, the prolonged use of DAPT was recommended. Overall, 235 patients, predominantly male (78.7%), with baseline characteristics exhibiting high rate of smoking (31.1%), diabetes (35.3%), and hypertension (32.8%) were found. The widely prescribed DAPT combination was aspirin with clopidogrel (72.3% at discharge and 46% on current use). Among all the enrolled patients, 163 patients were on DAPT while 71 were on single antiplatelet therapy (SAPT). A significant association between DAPT and PRECISE-DAPT scores was noted in terms of SAPT and DAPT. The appropriateness of DAPT was checked based on the scores, where 81% of the patients with DAPT ≥ 2 and 77.24% with PRECISE-DAPT score < 25 were appropriately prescribed with DAPT. The primary reason for drug interruptions was self-advised. The incidence of bleeding events was observed to be 7.23%, among which 5.1% had Type 1 bleeding according to BARC. Both DAPT and PRECISE-DAPT scores could be used to determine the appropriateness of the recommendations of DAPT in patients with AMI or undergoing PCI.
利用两种可用的预测模型,即双联抗血小板治疗(DAPT)评分和预测接受支架植入及后续双联抗血小板治疗患者出血并发症(PRECISE-DAPT)评分,我们旨在确定在接受经皮冠状动脉介入治疗(PCI)的急性心肌梗死(AMI)患者中DAPT的适宜性。我们回顾性纳入了235例AMI患者,并收集了所有患者的详细病史、危险因素和用药信息。计算了DAPT和PRECISE-DAPT评分。根据推荐的临界值对患者进行分组,并根据观察到的评分来衡量推荐的DAPT疗程的适宜性。采用出血学术研究联盟(BARC)分类来定义出血事件。在DAPT评分≥2且PRESICE-DAPT<25的患者中,建议延长DAPT使用时间。总体而言,共纳入235例患者,以男性为主(78.7%),基线特征显示吸烟率高(31.1%)、糖尿病(35.3%)和高血压(32.8%)。广泛使用的DAPT组合是阿司匹林联合氯吡格雷(出院时为72.3%,目前使用中为46%)。在所有纳入的患者中,163例接受DAPT治疗,71例接受单联抗血小板治疗(SAPT)。在SAPT和DAPT方面,DAPT与PRECISE-DAPT评分之间存在显著关联。根据评分检查DAPT的适宜性,其中DAPT评分≥2的患者中有81%以及PRECISE-DAPT评分<25的患者中有77.24%被适当开具了DAPT处方。药物中断的主要原因是患者自行决定。观察到出血事件的发生率为7.23%,其中根据BARC分类,5.1%为1型出血。DAPT和PRECISE-DAPT评分均可用于确定AMI患者或接受PCI患者中DAPT推荐的适宜性。