Sloan Gordon, Donatien Philippe, Privitera Rosario, Shillo Pallai, Caunt Sharon, Selvarajah Dinesh, Anand Praveen, Tesfaye Solomon
Division of Clinical Medicine, University of Sheffield, Sheffield, United Kingdom.
Diabetes Research Unit, Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, United Kingdom.
Front Pain Res (Lausanne). 2024 Oct 25;5:1485420. doi: 10.3389/fpain.2024.1485420. eCollection 2024.
Identifying distinct mechanisms and biomarkers for painful diabetic peripheral neuropathy (DPN) is required for advancing the treatment of this major global unmet clinical need. We previously provided evidence in calf skin biopsies that disproportion between reduced sensory small nerve fibers and increased blood vessels may distinguish painful from non-painful DPN. We proposed that overexposure of the reduced nerve fibers in DPN to increased hypoxemia-induced vasculature and related algogenic factors, e.g., nerve growth factor (NGF), leads to neuropathic pain. To further investigate this proposed mechanism, we have now studied more proximal thigh skin biopsies, to see if the same disproportion between increased vasculature and decreased nerve fibers generally differentiates painful DPN from painless DPN.
A total of 28 subjects with type 2 diabetes (T2DM) and 13 healthy volunteers (HV) underwent detailed clinical and neurophysiological assessments, based on the neuropathy composite score of the lower limbs [NIS(LL)] plus 7 tests. T2DM subjects were subsequently divided into three groups: painful DPN ( = 15), painless DPN ( = 7), and no DPN ( = 6). All subjects underwent skin punch biopsy from the upper lateral thigh 20 cm below the anterior iliac spine.
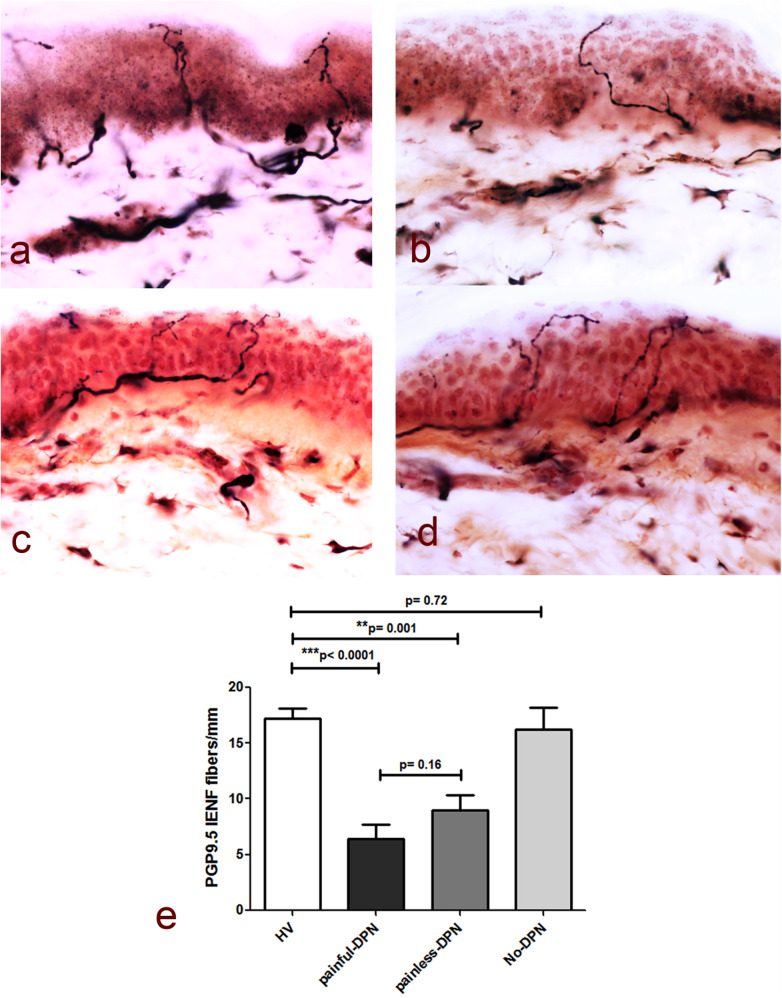
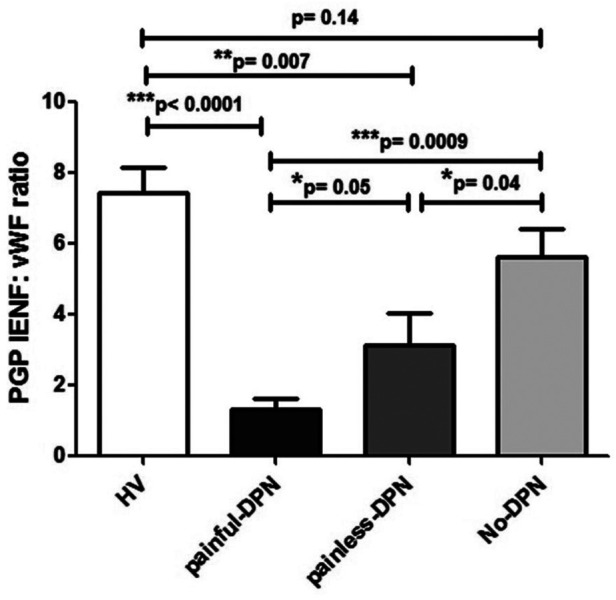
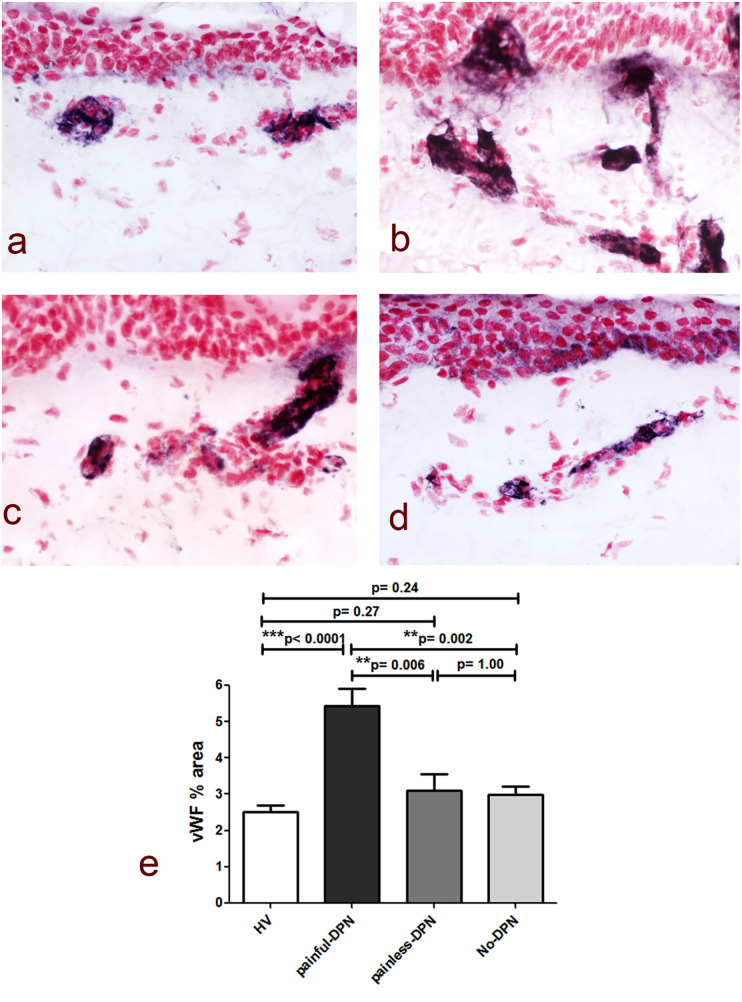
Skin biopsies showed decreased PGP 9.5-positive intraepidermal nerve fiber (IENF) density in both painful DPN ( < 0.0001) and painless DPN ( = 0.001). Vascular marker von Willebrand Factor (vWF) density was markedly increased in painful DPN vs. other groups, including painless DPN ( = 0.01). There was a resulting significant decrease in the ratio of intraepidermal nerve fiber density to vasculature and PGP9.5 to vWF, in painful DPN vs. painless DPN ( = 0.05). These results were similar in pattern to those observed in these HV and T2DM groups previously in distal calf biopsies; however, the increase in vWF was much higher and nerve fiber density much lower in the calf than thigh for painful DPN. Thigh skin vWF density was significantly correlated with several metabolic (waist/hip ratio, HbA1c), clinical (e.g., pain score), and neurophysiological measures.
This study supports our proposal that increased dermal vasculature, and its disproportionate ratio to reduced nociceptors, may help differentiate painful DPN from painless DPN. This disproportion is greater in the distal calf than the proximal thigh skin; hence, neuropathic pain in DPN is length-dependent and first localized to the distal lower limbs, mainly feet.
确定疼痛性糖尿病周围神经病变(DPN)的独特机制和生物标志物,对于满足这一全球主要未被满足的临床需求、推进其治疗至关重要。我们之前在小腿皮肤活检中发现,感觉小神经纤维减少与血管增多之间的失衡,可能是区分疼痛性与非疼痛性DPN的关键。我们推测,DPN中减少的神经纤维过度暴露于因低氧血症导致增加的血管系统及相关致痛因子,如神经生长因子(NGF),会引发神经病理性疼痛。为进一步探究这一推测机制,我们现在研究了更近端的大腿皮肤活检样本,以确定血管增多与神经纤维减少之间的相同失衡是否普遍可区分疼痛性DPN与无痛性DPN。
28名2型糖尿病(T2DM)患者和13名健康志愿者(HV)接受了详细的临床和神经生理学评估,评估基于下肢神经病变综合评分[NIS(LL)]加上7项测试。随后,T2DM患者被分为三组:疼痛性DPN(n = 15)、无痛性DPN(n = 7)和无DPN(n = 6)。所有受试者均在髂前上棘下方20 cm处的大腿外侧上部进行皮肤打孔活检。
皮肤活检显示,疼痛性DPN(P < 0.0001)和无痛性DPN(P = 0.001)的PGP 9.5阳性表皮内神经纤维(IENF)密度均降低。与其他组(包括无痛性DPN)相比,疼痛性DPN的血管标志物血管性血友病因子(vWF)密度显著增加(P = 0.01)。疼痛性DPN与无痛性DPN相比,表皮内神经纤维密度与血管系统以及PGP9.5与vWF的比值显著降低(P = 0.05)。这些结果在模式上与之前在小腿远端活检中观察到的HV和T2DM组相似;然而,对于疼痛性DPN,小腿的vWF增加幅度远高于大腿,神经纤维密度则远低于大腿。大腿皮肤vWF密度与多种代谢指标(腰臀比、糖化血红蛋白)、临床指标(如疼痛评分)和神经生理学指标显著相关。
本研究支持我们的观点,即真皮血管增多及其与伤害感受器减少的不成比例关系,可能有助于区分疼痛性DPN与无痛性DPN。这种失衡在小腿远端比大腿近端皮肤更明显;因此,DPN中的神经病理性疼痛具有长度依赖性,首先定位于下肢远端,主要是足部。