Anand Praveen, Privitera Rosario, Yiangou Yiangos, Donatien Philippe, Birch Rolfe, Misra Peter
Peripheral Neuropathy Unit, Centre for Clinical Translation, Hammersmith Hospital, Imperial College, London, United Kingdom.
Front Neurol. 2017 Sep 29;8:514. doi: 10.3389/fneur.2017.00514. eCollection 2017.
Trench foot, or non-freezing cold injury (NFCI), results from cold exposure of sufficient severity and duration above freezing point, with consequent sensory and vascular abnormalities which may persist for years. Based on observations of Trench foot in World War II, the condition was described as a vaso-neuropathy. While some reports have documented nerve damage after extreme cold exposure, sensory nerve fibres and vasculature have not been assessed with recent techniques in NFCI.
To assess patients with chronic sensory symptoms following cold exposure, in order to diagnose any underlying small fibre neuropathy, and provide insight into mechanisms of the persistent pain and cold hypersensitivity.
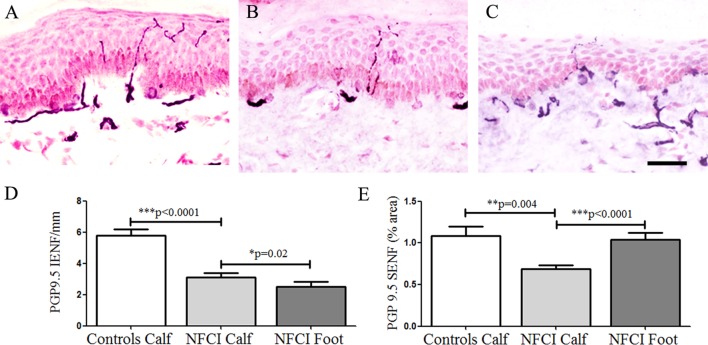
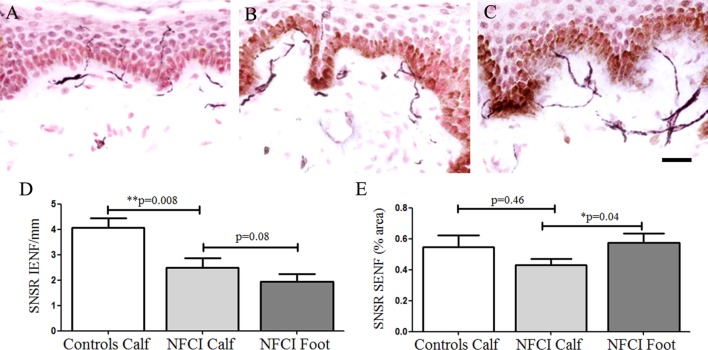
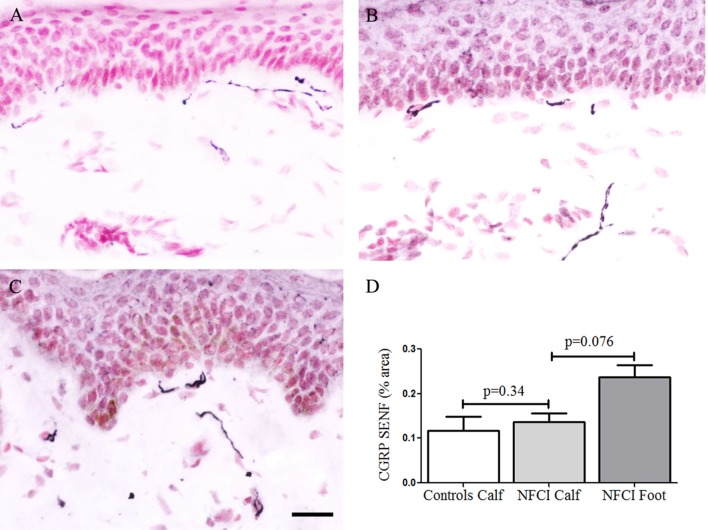
Thirty soldiers with cold exposure and persistent sensory symptoms (>4 months) were assessed with quantitative sensory testing, nerve conduction studies, and skin biopsies. Immunohistochemistry was used to assess intraepidermal (IENF) and subepidermal (SENF) nerve fibres with a range of markers, including the pan-neuronal marker protein gene product 9.5 (PGP 9.5), regenerating fibres with growth-associated protein 43 (GAP43), and nociceptor fibres with transient receptor potential cation channel subfamily V member 1 (TRPV1), sensory neuron-specific receptor (SNSR), and calcitonin gene-related peptide (CGRP). von Willebrand factor (vWF), endothelial nitric oxide synthase (eNOS), and vascular endothelial growth factor (VEGF) were used for assessing blood vessels, and transient receptor potential cation channel, subfamily A member 1 (TRPA1) and P2X purinoceptor 7 (P2X7) for keratinocytes, which regulate nociceptors release of nerve growth factor.
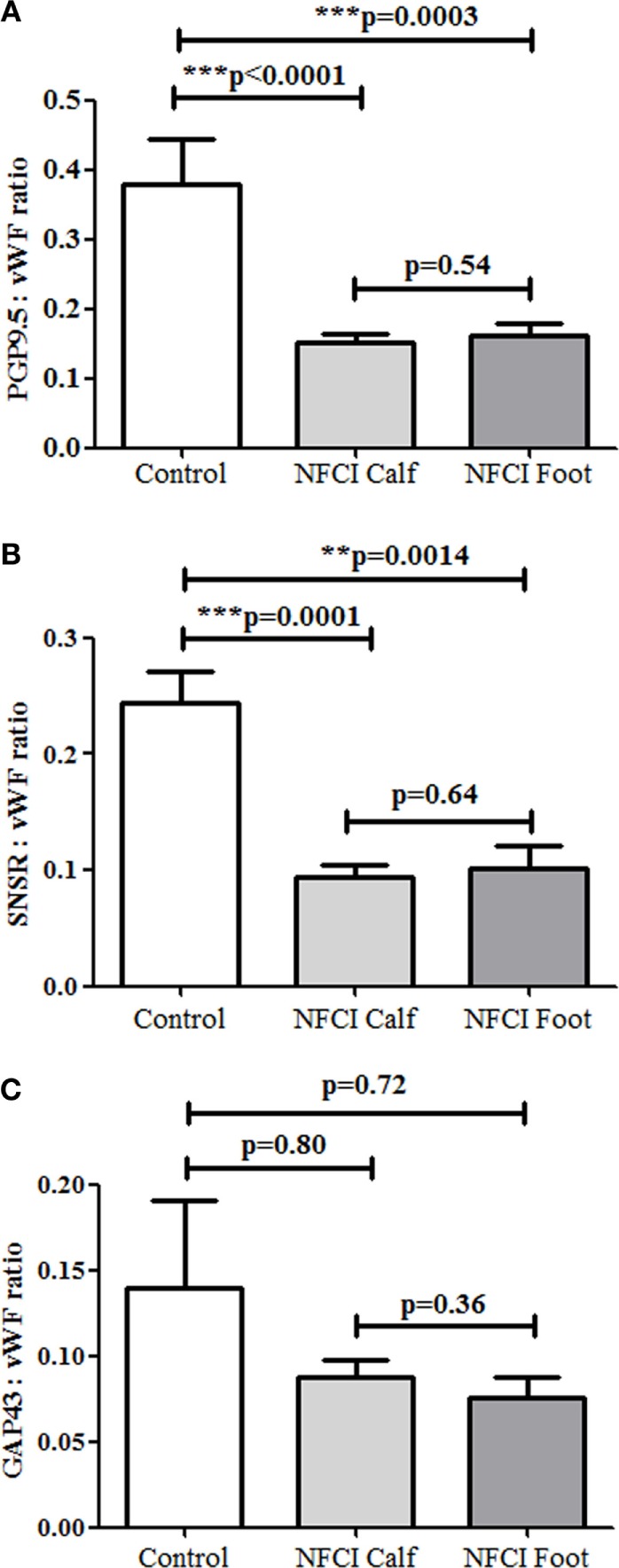
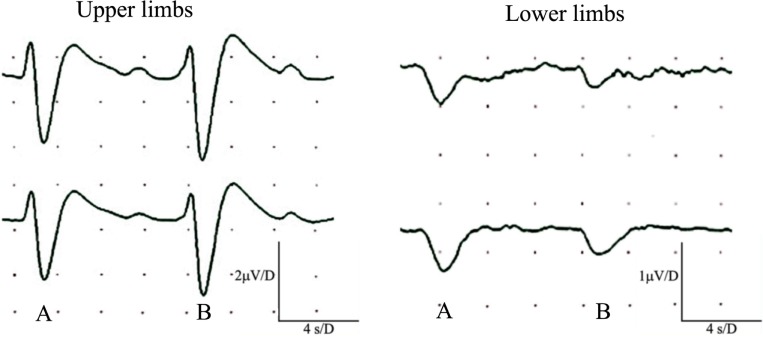
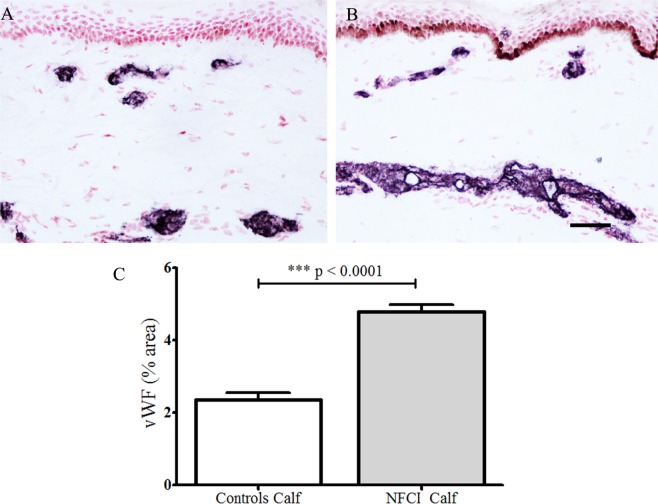
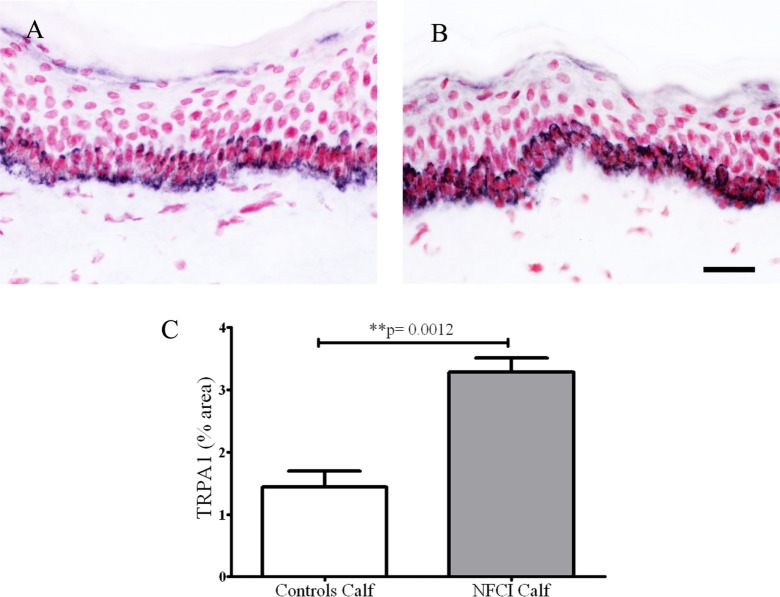
Clinical examination showed pinprick sensation was abnormal in the feet of 20 patients (67%), and between 67 and 83% had abnormalities of thermal thresholds to the different modalities. 7 patients (23%) showed reduced sensory action potential amplitude of plantar nerves. 27 patients (90%) had decreased calf skin PGP 9.5 IENF ( < 0.0001), the remaining 3 patients had decreased nerve markers in subepidermis or foot skin. There were marked increases of all vascular markers (for vWF in calf skin, < 0.0001), and increased sensory or regenerating SENF (for calf skin, GAP43, = 0.002). TRPA1 ( = 0.0012) and P2X7 ( < 0.0001) were increased in basal keratinocytes.
A range of skin biopsy markers and plantar nerve conduction studies are useful objective assessments for the diagnosis of peripheral neuropathy in NFCI. Our results suggest that an increase in blood vessels following tissue ischaemia/hypoxia could be associated with disproportionate and abnormal nerve fibres (irritable nociceptors), and may lead to NFCI as a "painful vaso-neuropathy."
战壕足,即非冻结性冷损伤(NFCI),是由于在冰点以上受到足够严重和持续时间的寒冷暴露所致,随之产生的感觉和血管异常可能会持续数年。基于二战期间对战壕足的观察,该病被描述为一种血管神经病变。虽然一些报告记录了极端寒冷暴露后的神经损伤,但在NFCI中,感觉神经纤维和脉管系统尚未采用最新技术进行评估。
评估寒冷暴露后出现慢性感觉症状的患者,以诊断任何潜在的小纤维神经病变,并深入了解持续性疼痛和冷超敏反应的机制。
对30名有寒冷暴露史且存在持续性感觉症状(超过4个月)的士兵进行了定量感觉测试、神经传导研究和皮肤活检。免疫组织化学方法用于用一系列标志物评估表皮内(IENF)和表皮下(SENF)神经纤维,包括泛神经元标志物蛋白基因产物9.5(PGP 9.5)、具有生长相关蛋白43(GAP43)的再生纤维,以及具有瞬时受体电位阳离子通道亚家族V成员1(TRPV1)、感觉神经元特异性受体(SNSR)和降钙素基因相关肽(CGRP)的伤害性感受器纤维。血管性血友病因子(vWF)、内皮型一氧化氮合酶(eNOS)和血管内皮生长因子(VEGF)用于评估血管,瞬时受体电位阳离子通道亚家族A成员1(TRPA1)和P2X嘌呤受体7(P2X7)用于评估角质形成细胞,角质形成细胞调节伤害性感受器释放神经生长因子。
临床检查显示,20名患者(67%)足部的针刺感觉异常,67%至83%的患者对不同刺激方式的热阈值存在异常。7名患者(23%)显示足底神经感觉动作电位幅度降低。27名患者(90%)小腿皮肤的PGP 9.5 IENF减少(P<0.0001),其余3名患者表皮下或足部皮肤的神经标志物减少。所有血管标志物均显著增加(小腿皮肤vWF,P<0.0001),感觉或再生SENF增加(小腿皮肤GAP43,P=0.002)。基底角质形成细胞中的TRPA1(P=0.0012)和P2X7(P<0.0001)增加。
一系列皮肤活检标志物和足底神经传导研究是诊断NFCI外周神经病变的有用客观评估方法。我们的结果表明,组织缺血/缺氧后血管增加可能与不成比例和异常的神经纤维(易激惹的伤害性感受器)有关,并可能导致NFCI成为一种“疼痛性血管神经病变”。