Motta Rodrigo V, Gupta Vipin, Hartery Karen, Bassett Paul, Leedham Simon J, Chapman Roger W, Travis Simon Pl, Culver Emma L, East James E
Translational Gastroenterology and Liver Unit, Experimental Medicine Division, Nuffield Department of Medicine, University of Oxford, Oxford, United Kingdom of Great Britain and Northern Ireland.
Department of Gastroenterology, North Bristol NHS Trust, Bristol, United Kingdom of Great Britain and Northern Ireland.
Endosc Int Open. 2024 Nov 11;12(11):E1285-E1294. doi: 10.1055/a-2437-8102. eCollection 2024 Nov.
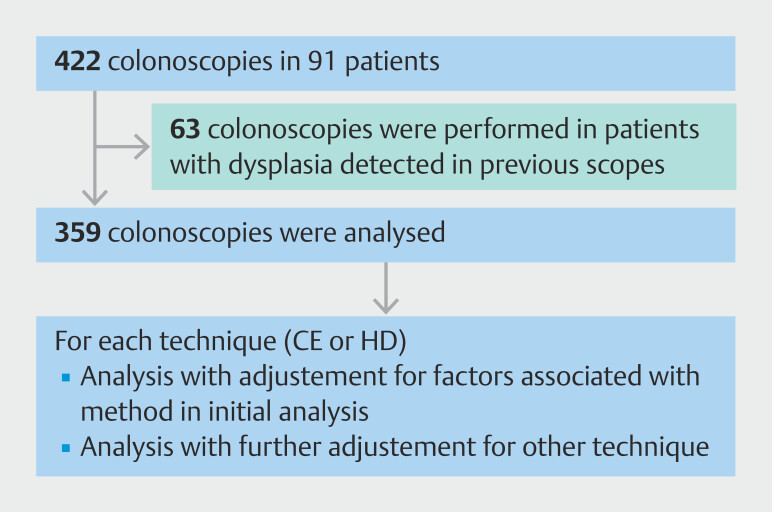
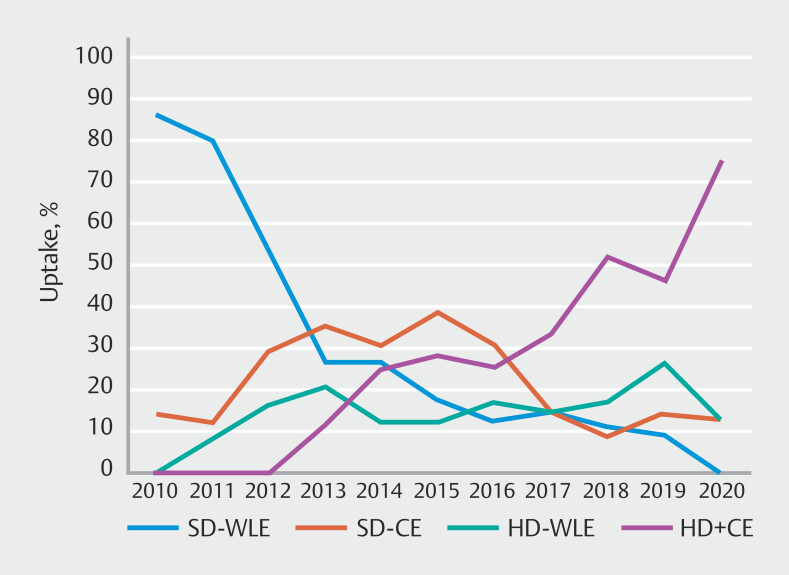
Patients with primary sclerosing cholangitis and inflammatory bowel disease (IBD) have a high risk of colorectal cancer. There is no agreement on the best technique for surveillance for colorectal neoplasia. We aimed to assess whether chromoendoscopy and/or high-definition endoscopy is associated with increased detection of neoplasia in patients with primary sclerosing cholangitis undergoing surveillance compared with when they were not used. This was a single-center, retrospective, observational study designed to analyze differences in the detection of neoplasia (adenomatous and serrated) among patients with primary sclerosing cholangitis and IBD who underwent annual surveillance between 2010 and 2020. Multilevel logistic regression was used to adjust for confounders. Ninety-one patients were identified, resulting in 359 colonoscopies with 360 person-years of follow up. Over the study period, 22 of 91 patients (24%) had at least one neoplastic lesion identified; however, the mean neoplastic lesion rate was 0.87 (54/63) for the primary sclerosing cholangitis-ulcerative colitis subgroup compared with 0.24 (4/17) for the primary sclerosing cholangitis-Crohn's disease subgroup. Chromoendoscopy was associated with a significantly higher detection rate for neoplasia (odds ratio [OR] 5.58, 95% confidence interval [CI] 2.08-14.9, =0.001), and this association remained after adjusting for confounders, including high-definition endoscopy. High-definition endoscopes had a higher rate of neoplasia detection, but the significance was lost after adjustment for confounders, including chromoendoscopy (OR 1.93, 95% CI 0.69-5.40, =0.21). Chromoendoscopy is associated with a higher detection rate for neoplasia in patients with primary sclerosing cholangitis and IBD even with high-definition colonoscopes.
原发性硬化性胆管炎和炎症性肠病(IBD)患者患结直肠癌的风险很高。对于结直肠肿瘤的最佳监测技术尚无共识。我们旨在评估与未使用相比,染色内镜检查和/或高清内镜检查是否与接受监测的原发性硬化性胆管炎患者肿瘤的检出率增加相关。这是一项单中心、回顾性、观察性研究,旨在分析2010年至2020年间接受年度监测的原发性硬化性胆管炎和IBD患者中肿瘤(腺瘤性和锯齿状)检出率的差异。采用多水平逻辑回归对混杂因素进行校正。共纳入91例患者,进行了359次结肠镜检查,随访360人年。在研究期间,91例患者中有22例(24%)至少发现一处肿瘤病变;然而,原发性硬化性胆管炎-溃疡性结肠炎亚组的平均肿瘤病变率为0.87(54/63),而原发性硬化性胆管炎-克罗恩病亚组为0.24(4/17)。染色内镜检查与肿瘤的显著更高检出率相关(优势比[OR]5.58,95%置信区间[CI]2.08-14.9,P=0.001),在对包括高清内镜检查在内的混杂因素进行校正后,这种关联仍然存在。高清内镜检查的肿瘤检出率较高,但在对包括染色内镜检查在内的混杂因素进行校正后,其显著性消失(OR 1.93,95%CI 0.69-5.40,P=0.21)。即使使用高清结肠镜,染色内镜检查也与原发性硬化性胆管炎和IBD患者的肿瘤更高检出率相关。