Nishimura Akinobu, Fujikawa Yuki, Senga Yoshiyuki, Nakazora Shigeto, Konno Chihiro, Sudo Akihiro
Department of Orthopaedic and Sports Medicine, Mie University Graduate School of Medicine, Tsu, Japan.
Department of Orthopaedic Surgery, Mie University Graduate School of Medicine, Tsu, Japan.
Ann Jt. 2024 Aug 30;9:40. doi: 10.21037/aoj-24-10. eCollection 2024.
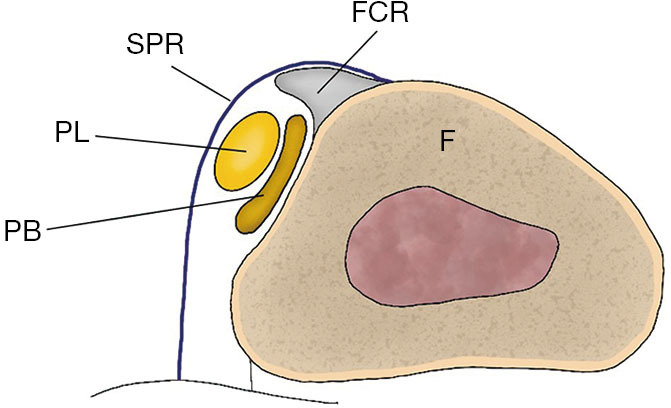
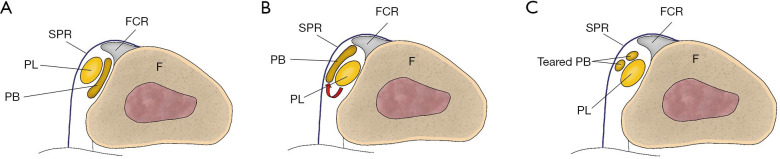
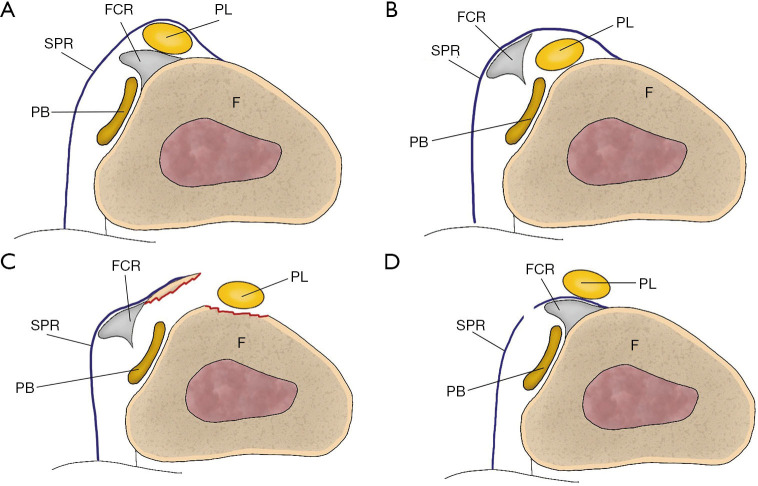
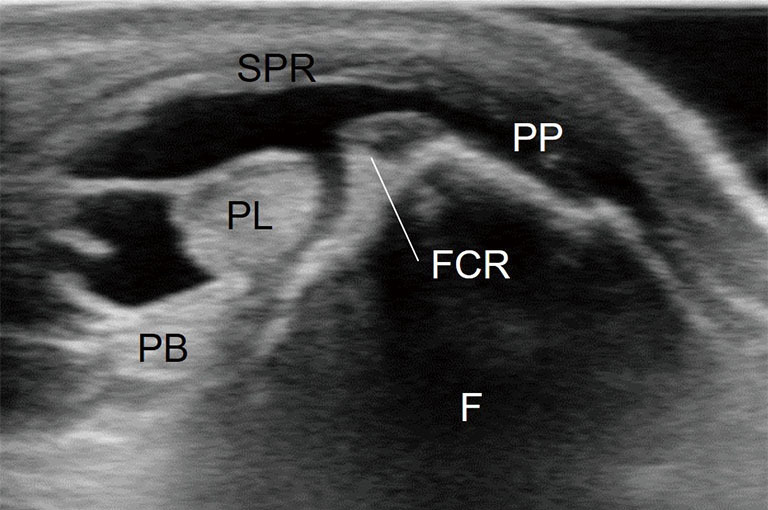
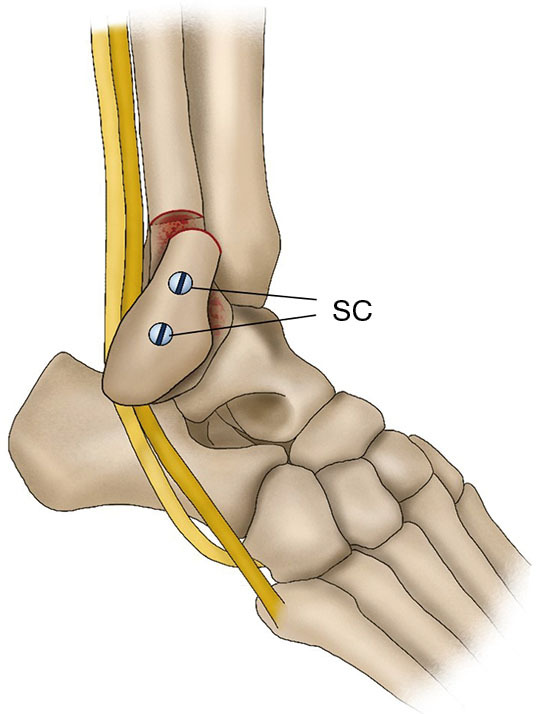
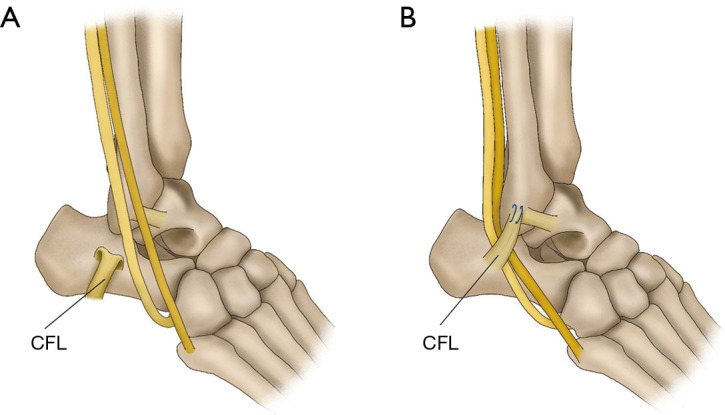
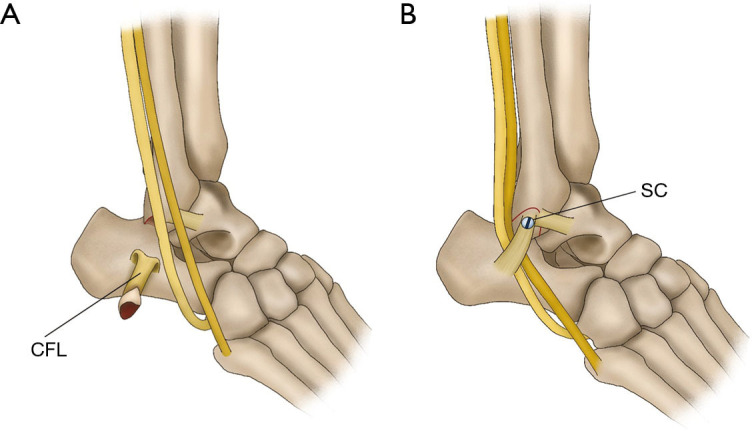
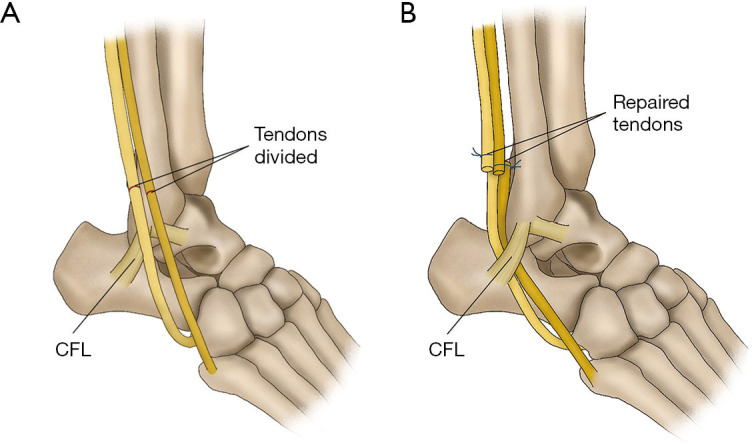
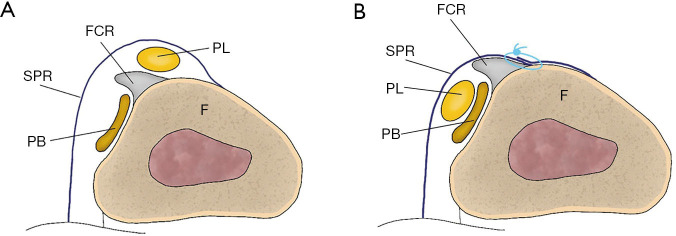
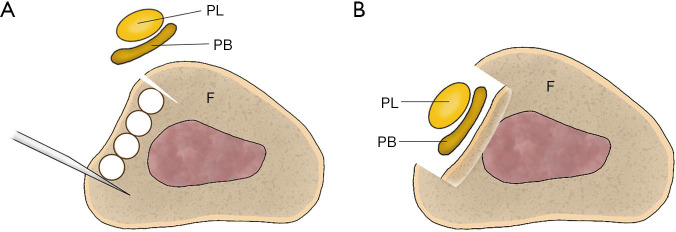
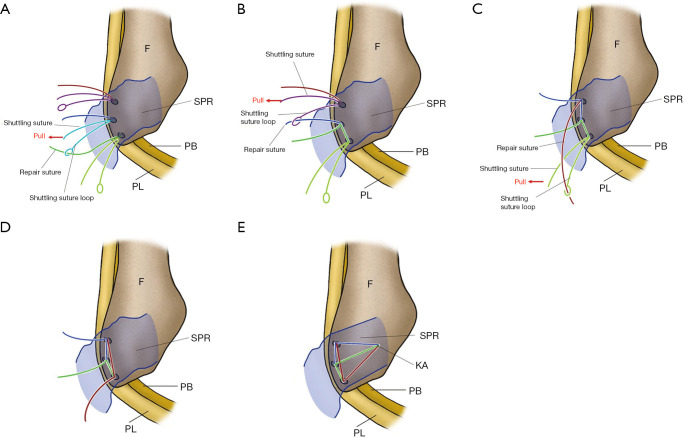
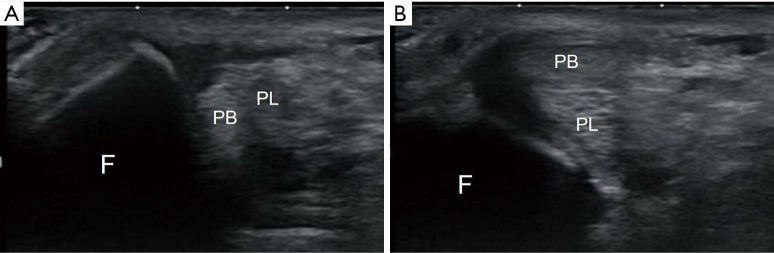
The peroneus muscles, consisting of the peroneus longus (PL) and peroneus brevis (PB) tendons, are vulnerable to injury at anatomically specific sites or within tendon sheaths. Peroneal tendon dislocation (PTD) is often misdiagnosed as a lateral ankle sprain as it occurs at a lower frequency than a lateral ankle sprain. Anatomical variations in the retromalleolar groove, soft tissue overstuffing, and presence of accessory peroneal muscles contribute to the etiology of PTD. PTD has been classified into four types based on injury patterns involving the superior peroneal retinaculum (SPR) and fibrocartilaginous ridge. Diagnosis involves recognizing tender points and using imaging including magnetic resonance imaging (MRI) and ultrasonography. Conservative treatments, including below-knee plaster casts, have varying success rates, and some patients progress to recurrent PTD (RPTD), prompting consideration of surgical interventions. Diagnosis is easy in patients with RPTD who can reproduce the dislocation by themselves; however, in many cases, this is not possible. In such cases, ultrasonography after intrasheath injection is effective in confirming the presence of a pseudo-pouch. RPTD can be diagnosed if a pseudo-pouch is identified during ultrasonography. Surgical approaches such as osteotomy, soft tissue procedures, and groove deepening techniques are used to stabilize the peroneal tendons. Soft tissue procedures, especially SPR reattachment, have emerged as a preferred option, demonstrating outcomes comparable to those of osteotomy, with fewer complications. Intrasheath subluxation, a unique PTD subtype, is diagnosed using ultrasonography. In this type of subluxation, no damage to the SPR is observed, and the positions of the PL and PB tendons are interchanged. Surgical intervention may involve excision of the synovium and SPR repair. In cases of PTD complicated by a longitudinal rupture of the PB tendon, suturing of the torn area or tubularization of the remaining tendon for partial resection of the degenerated tendon can be performed. The purpose of this article is to describe the methods for diagnoses and management of PTD.
腓骨肌由腓骨长肌(PL)和腓骨短肌(PB)肌腱组成,在解剖学特定部位或腱鞘内易受损伤。腓骨肌腱脱位(PTD)常被误诊为外侧踝关节扭伤,因为其发生频率低于外侧踝关节扭伤。外踝后沟的解剖变异、软组织填充过多以及副腓骨肌的存在是PTD病因的一部分。根据涉及腓骨上支持带(SPR)和纤维软骨嵴的损伤模式,PTD已被分为四种类型。诊断包括识别压痛点并使用包括磁共振成像(MRI)和超声检查在内的影像学检查。保守治疗,包括膝下石膏固定,成功率各不相同,一些患者会发展为复发性PTD(RPTD),从而促使考虑手术干预。对于能够自行重现脱位的RPTD患者,诊断很容易;然而,在许多情况下,这是不可能的。在这种情况下,鞘内注射后的超声检查对于确认假囊的存在是有效的。如果在超声检查中发现假囊,则可诊断为RPTD。手术方法如截骨术、软组织手术和沟加深技术用于稳定腓骨肌腱。软组织手术,尤其是SPR重新附着,已成为首选方案,其疗效与截骨术相当,并发症更少。鞘内半脱位是一种独特的PTD亚型,通过超声检查进行诊断。在这种半脱位类型中,未观察到SPR损伤,PL和PB肌腱的位置互换。手术干预可能包括滑膜切除和SPR修复。在PTD合并PB肌腱纵向断裂的情况下,可以对撕裂区域进行缝合或对剩余肌腱进行管状化以部分切除退变的肌腱。本文的目的是描述PTD的诊断和管理方法。