Domenech Carine, Kicinski Michal, De Moerloose Barbara, Piette Caroline, Chahla Wadih A, Kornreich Laure, Pasquet Marlène, Uyttebroeck Anne, Theron Alexandre, Poirée Marilyne, Arfeuille Chloé, Bakkus Marleen, Grardel Nathalie, Paillard Catherine, Freycon Claire, Millot Frédéric, Simon Pauline, Philippet Pierre, Pluchart Claire, Suciu Stefan, Rohrlich Pierre, Ferster Alina, Bertrand Yves, Cavé Hélène
Department of Pediatric Hematology-Oncology, Institut d'Hématologie et d'Oncologie Pédiatrique, Hospices Civils de Lyon Université Lyon1 Lyon France.
Department of Statistic EORTC Headquarters Brussels Belgium.
Hemasphere. 2024 Nov 13;8(11):e70025. doi: 10.1002/hem3.70025. eCollection 2024 Nov.
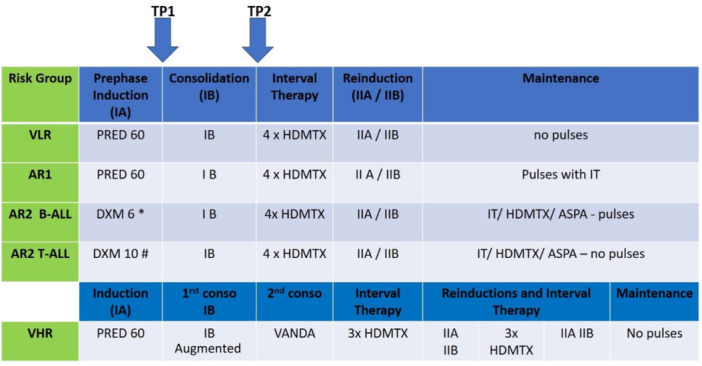
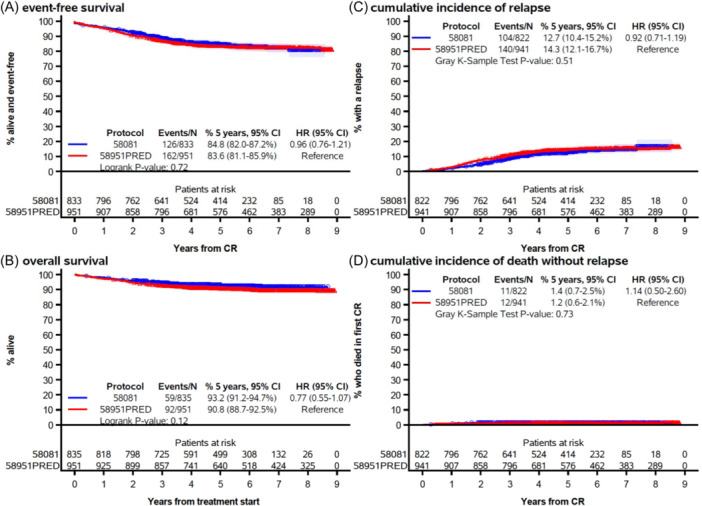
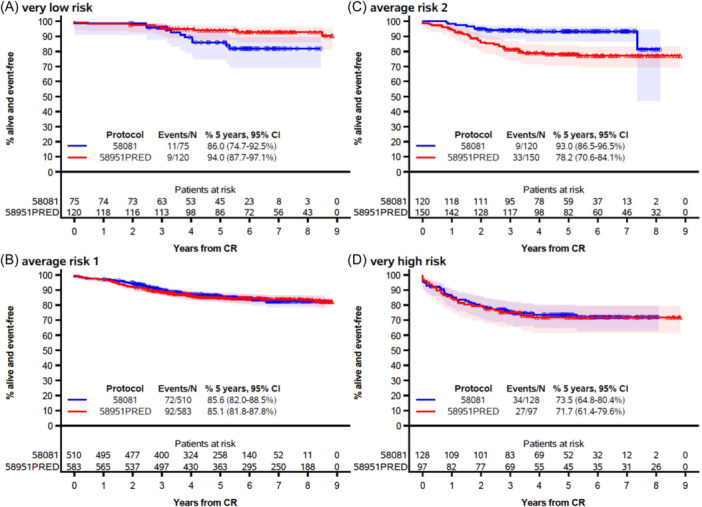
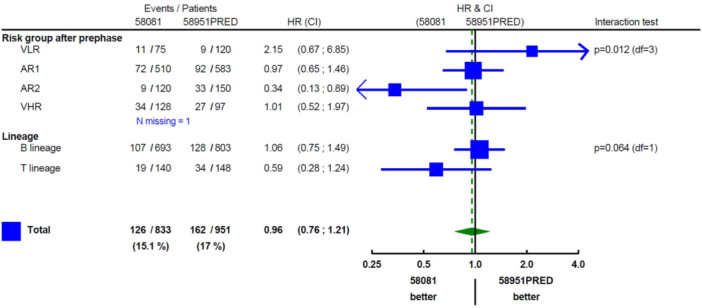
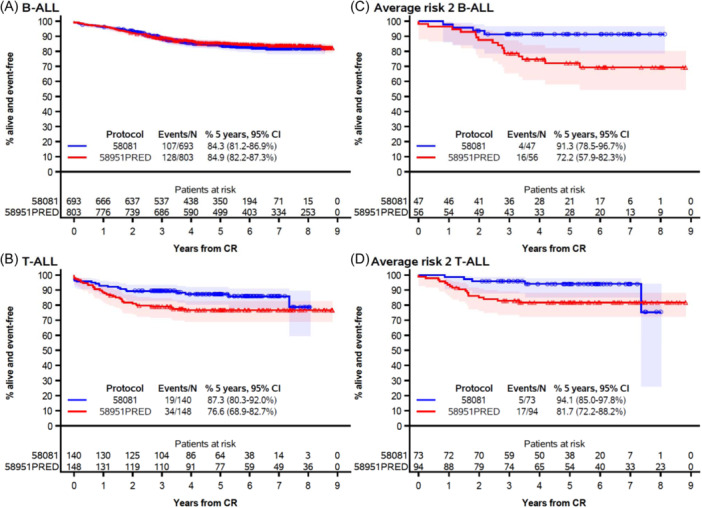
Here, we report the results of the prospective cohort study EORTC-CLG 58081 and compare them to the control arm of the randomized phase 3 trial EORTC-CLG 58951, on which treatment recommendations were built. In both studies, patients aged 1-18 years with negative acute lymphoblastic leukemia of the B-lineage (B-ALL) or T-lineage (T-ALL) were treated using a BFM backbone without cranial irradiation. Similarly to the control arm of 58951, prednisolone (PRED) 60 mg/m/day was used for induction therapy, but a few modifications were made. Dexamethasone (DXM) was used in average-risk 2 (AR2) T-ALL and B-ALL during induction, 10 and 6 mg/m/day, respectively. Leucovorin rescue was delayed to 42 h instead of 36 h after initiation of high-dose methotrexate, and a postconsolidation MRD time point was added to stratify patients. Between 2011 and 2017, 835 patients were prospectively enrolled in the 58081 study. Overall, the 5-year event-free survival (EFS) was 84.8% versus 83.6% (hazard ratio [HR], 0.96 [95% confidence interval [CI]: 0.76-1.21]) for 58081 versus 58951 considered as a control group, respectively, 84.3% versus 84.9% (HR, 1.06 [99% CI: 0.75-1.49]) in B-ALL but 87.3% versus 76.6% (HR, 0.59 [99% CI: 0.28-1.24]) in T-ALL. The comparison between the two studies regarding EFS differed by risk group ( = 0.012). The HR was 2.15 (99% CI: 0.67-6.85) for very low-risk but 0.34 (99% CI: 0.13-0.89) for AR2. The particularly favorable results observed in the T-ALLs and AR2 subgroups suggest the benefit of using DXM in specific patient groups and highlight the importance of risk stratification.
在此,我们报告了前瞻性队列研究EORTC-CLG 58081的结果,并将其与随机3期试验EORTC-CLG 58951的对照组进行比较,后者是制定治疗建议的依据。在这两项研究中,年龄在1至18岁、B系(B-ALL)或T系(T-ALL)急性淋巴细胞白血病阴性的患者均采用不含颅脑照射的BFM方案进行治疗。与58951的对照组类似,诱导治疗使用泼尼松龙(PRED)60mg/m²/天,但做了一些调整。诱导期间,中危2(AR2)T-ALL和B-ALL分别使用地塞米松(DXM),剂量为10mg/m²/天和6mg/m²/天。亚叶酸钙解救延迟至高剂量甲氨蝶呤开始后42小时而非36小时,并增加了巩固后微小残留病(MRD)时间点以对患者进行分层。2011年至2017年期间,835例患者前瞻性纳入58081研究。总体而言,58081研究与作为对照组的58951研究相比,5年无事件生存率(EFS)分别为84.8%和83.6%(风险比[HR],0.96[95%置信区间[CI]:0.76 - 1.21]),在B-ALL中分别为84.3%和84.9%(HR,1.06[99%CI:0.75 - 1.49]),但在T-ALL中分别为87.3%和76.6%(HR,0.59[99%CI:0.28 - 1.24])。两项研究在EFS方面的比较因风险组而异(P = 0.012)。极低风险组的HR为2.15(99%CI:0.67 - 6.85),而AR2组为0.34(99%CI:0.13 - 0.89)。在T-ALL和AR2亚组中观察到的特别良好结果表明在特定患者组中使用DXM的益处,并突出了风险分层的重要性。