Ramaswamy Tara, DeWane Michael P, Dashti Hassan S, Lau Meghan, Wischmeyer Paul E, Nagrebetsky Alexander, Sparling Jamie
Department of Anesthesia, Critical Care and Pain Medicine, Massachusetts General Hospital, Boston, MA, United States.
Department of Surgery, Division of Trauma, Emergency Surgery & Surgical Critical Care, Massachusetts General Hospital, Boston, MA, United States.
Adv Nutr. 2025 Jan;16(1):100345. doi: 10.1016/j.advnut.2024.100345. Epub 2024 Nov 17.
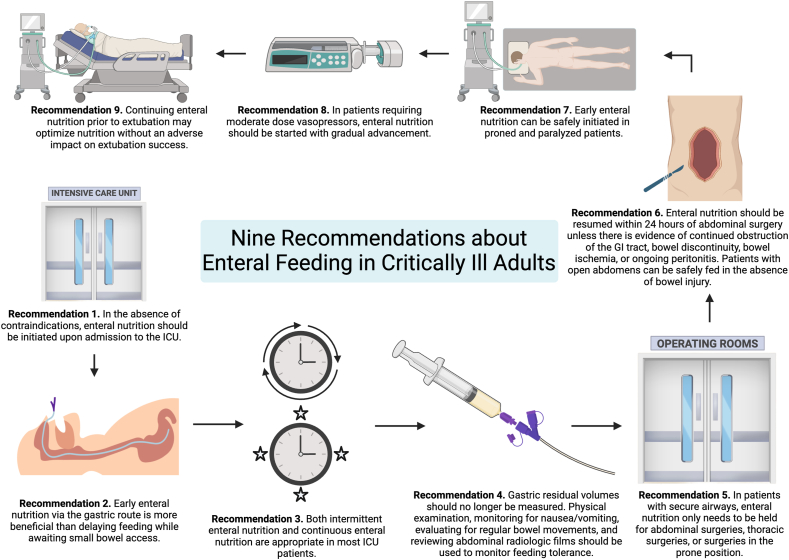
Malnutrition is a well-studied and significant prognostic risk factor for morbidity and mortality in critically ill perioperative patients. Common nutrition myths in the critically ill may prevent early, consistent, and adequate delivery of enteral nutrition. We outlined 9 common intensive care unit (ICU) nutrition misconceptions and our recommendations to optimize enteral nutrition in critically ill patients based on the review of available literature. Our approach is to treat every patient admitted to the ICU as at risk for malnutrition and to initiate enteral nutrition upon admission in the absence of contraindications. Early enteral nutrition via the gastric route is more beneficial than delaying feeding while awaiting small bowel access and daytime-intermittent nutrition support can safely be initiated over continuous feeding. Gastric residual volumes to assess feeding tolerance should no longer be routinely measured. For perioperative nutrition, we recommend continuing enteral nutrition for most patients with secure airways undergoing anesthesia and resuming nutrition within 24 h of abdominal surgery; even patients with open abdomens can be safely fed in the absence of bowel injury. Critically ill patients who are proned, paralyzed, and on vasopressors can usually continue enteral nutrition. Finally, continuing enteral nutrition before extubation may optimize nutrition without compromising extubation success. In this review, we highlight several common misconceptions regarding ICU nutrition that may prevent achieving nutrition goals and subsequently lead to increased malnutrition, morbidity, and mortality. This knowledge may contribute to increased implementation of early and consistent enteral nutrition strategies to improve outcomes in critically ill adult patients.
营养不良是围手术期重症患者发病和死亡的一个经过充分研究且重要的预后风险因素。重症患者中常见的营养误区可能会阻碍肠内营养的早期、持续和充分供给。基于对现有文献的综述,我们概述了9个常见的重症监护病房(ICU)营养误区以及我们对优化重症患者肠内营养的建议。我们的方法是将每一位入住ICU的患者视为有营养不良风险的患者,并且在没有禁忌证的情况下入院时即开始肠内营养。经胃途径的早期肠内营养比等待小肠通路时延迟喂养更有益,并且日间间歇营养支持可以安全地在持续喂养之上启动。用于评估喂养耐受性的胃残余量不应再常规测量。对于围手术期营养,我们建议大多数气道安全的患者在麻醉期间继续肠内营养,并在腹部手术后24小时内恢复营养;即使是腹部开放的患者,在没有肠损伤的情况下也可以安全喂养。俯卧、瘫痪且使用血管活性药物的重症患者通常可以继续肠内营养。最后,在拔管前继续肠内营养可能会优化营养状况,而不会影响拔管成功率。在本综述中,我们强调了几个关于ICU营养的常见误区,这些误区可能会妨碍实现营养目标,并随后导致营养不良、发病率和死亡率增加。这些知识可能有助于增加早期和持续肠内营养策略的实施,以改善成年重症患者的预后。