Department of Radiology and Neuroradiology, University Hospital Schleswig-Holstein, Campus Kiel Arnold-Heller-Str. 3, Haus C/D, D-24105, Kiel, Germany.
Sci Rep. 2024 Nov 18;14(1):28397. doi: 10.1038/s41598-024-78789-2.
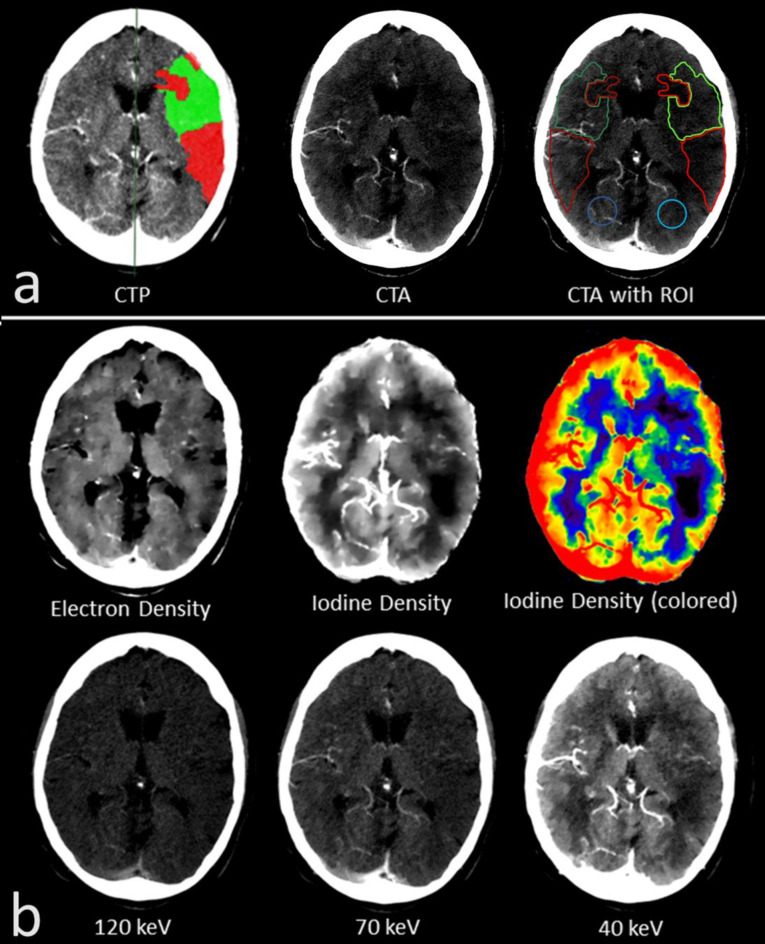
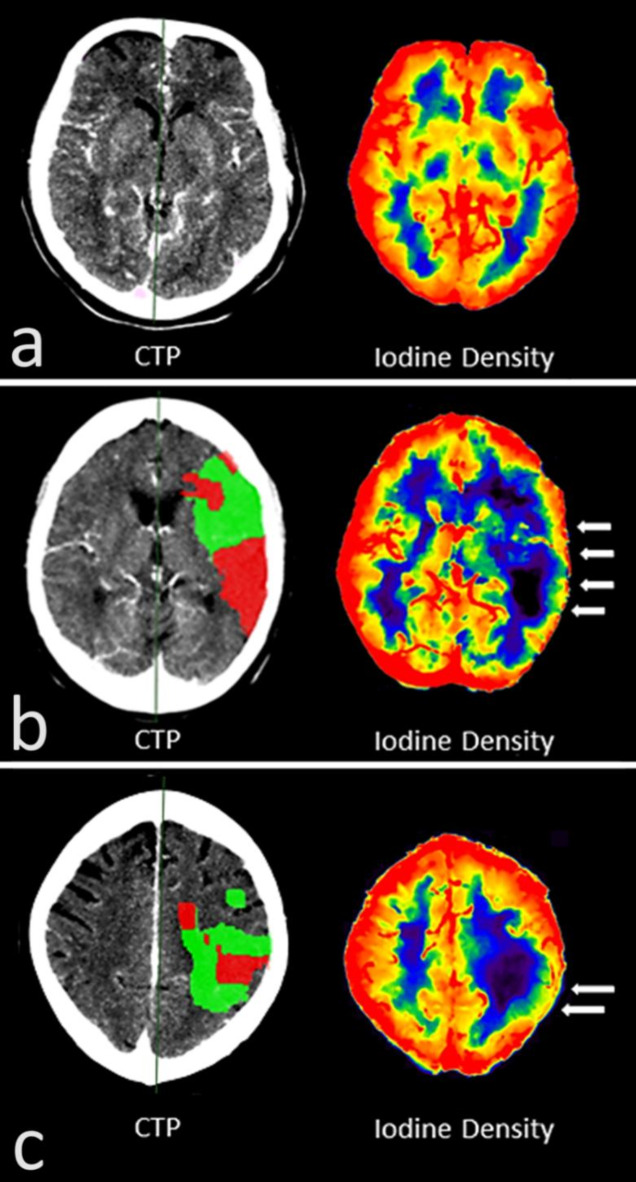
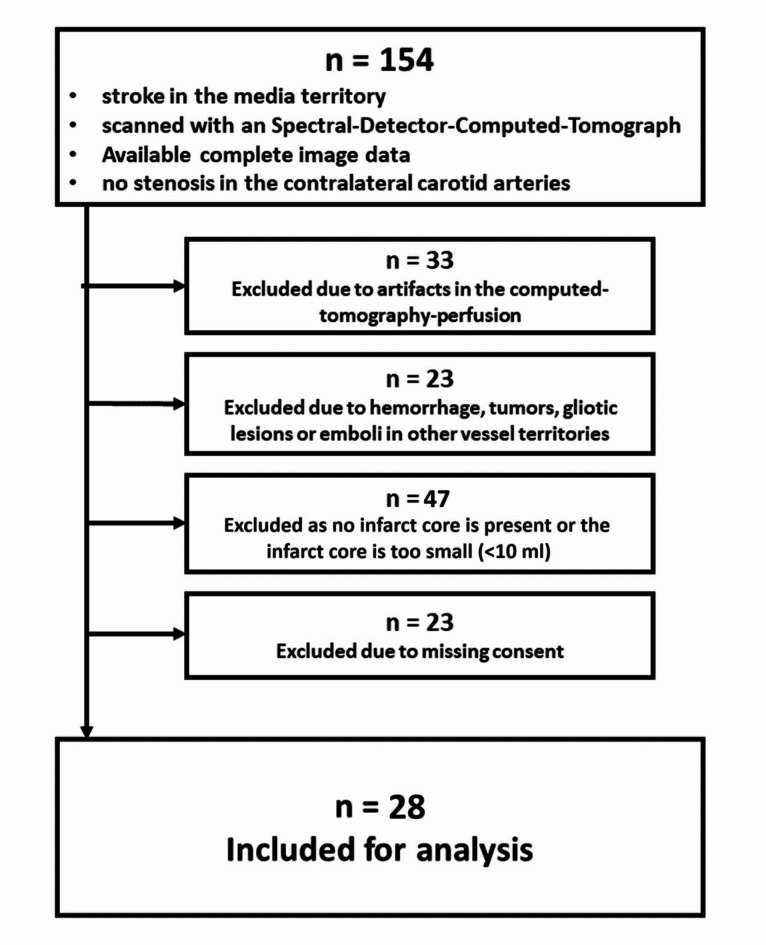
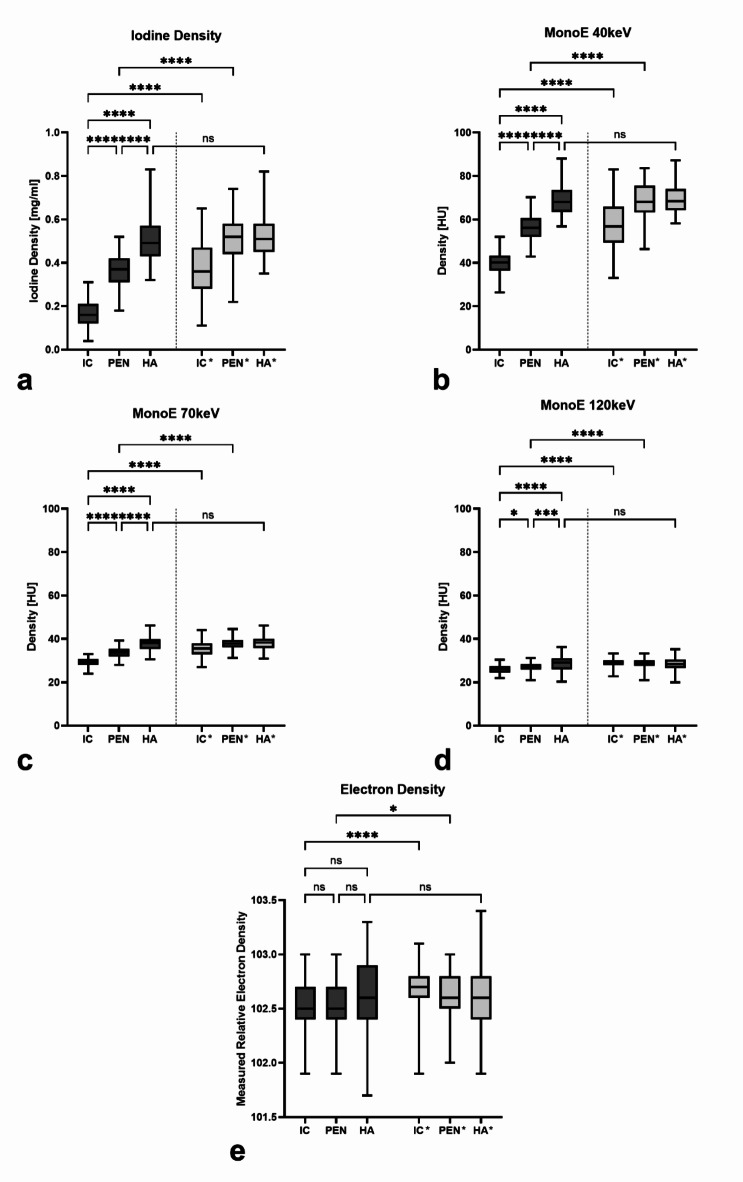
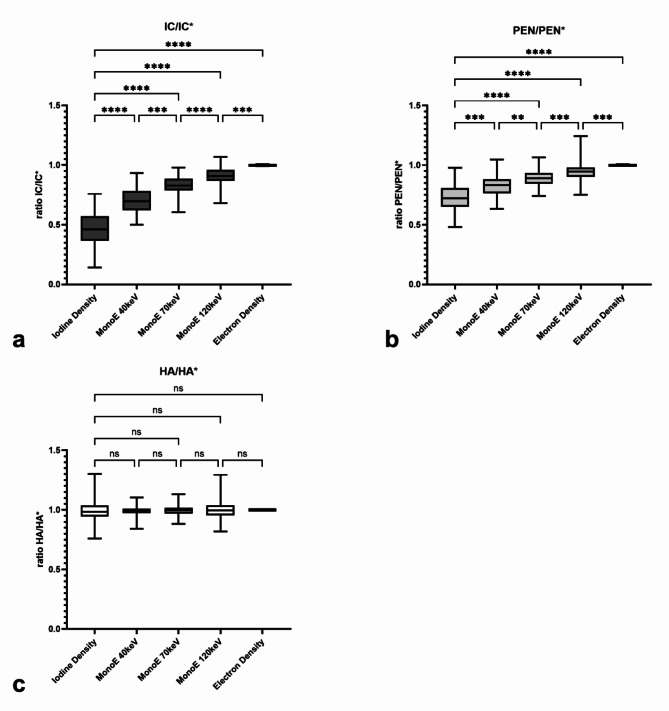
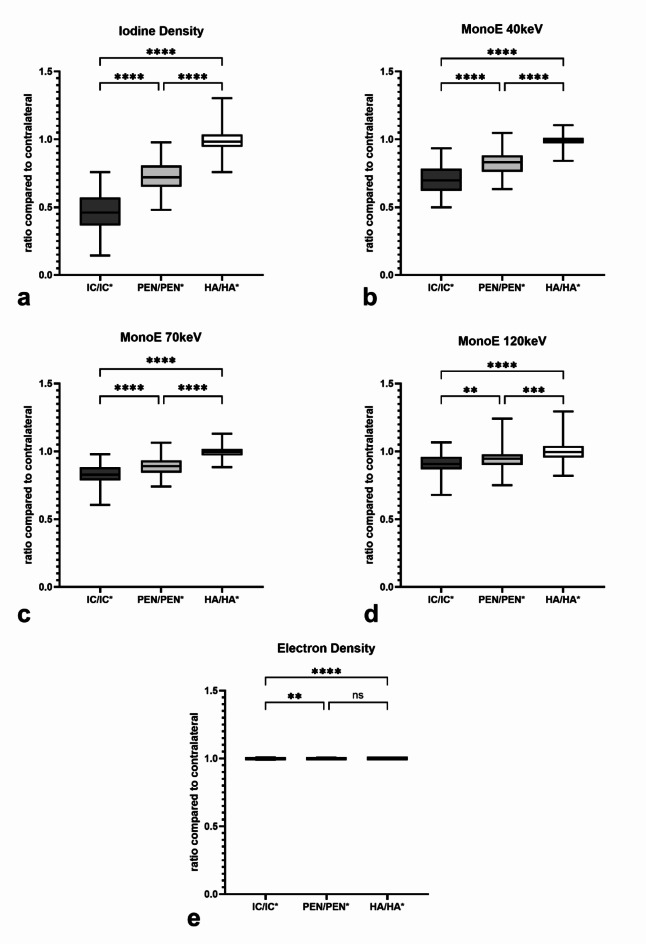
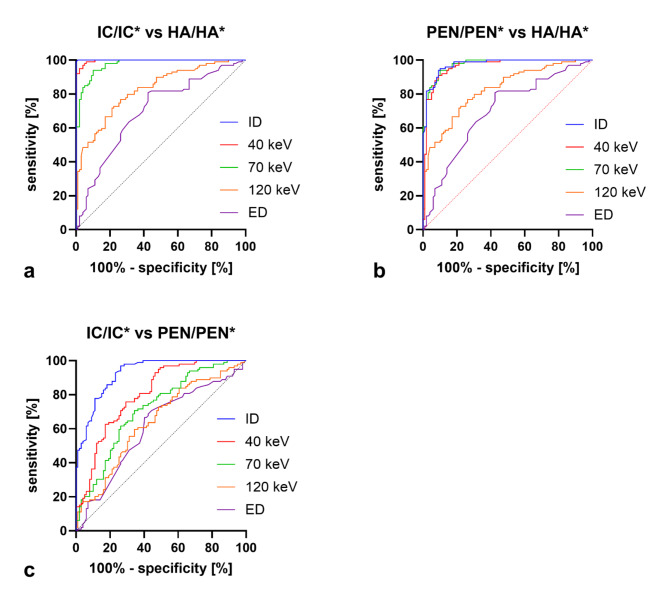
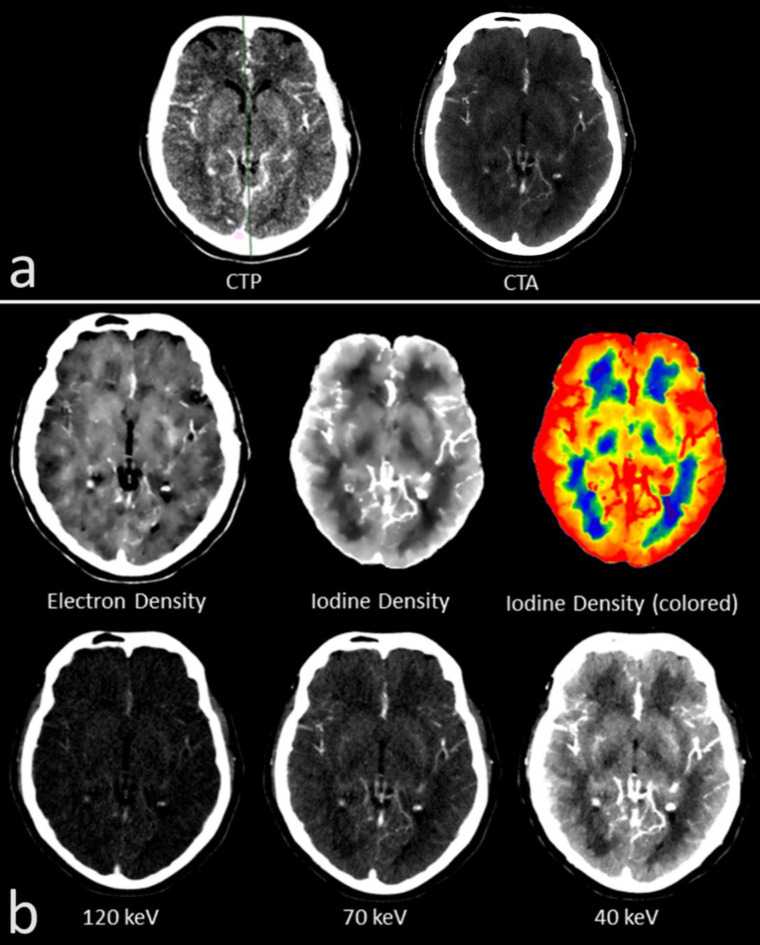
Acute stroke imaging includes native CT, CT-angiography (CTA), and CT-perfusion (CTP). CTP assesses the irreversibly damaged infarct core (IC), and the potentially salvageable penumbra (PEN) and distinguishes these from areas of healthy parenchyma (HA). However, it requires additional contrast agent and radiation. Spectral-CT (SCT) enables spectral imaging like e.g., iodine-density imaging, and we evaluated its potential in estimating IC and PEN using monophasic CTA data only. We analysed 28 patients with mediainfarction. CTP-analysis derived areas of IC, PEN and HA on infarction side, as well as their healthy hemisphere's counterparts were transferred to CTA as Region of interest (ROI). Spectral measurements included Hounsfield-Units in monoenergetic maps (MonoE) at 40 keV, 70 keV, and 120 keV, plus iodine-density (ID) and electron-density (ED) values, totalling 2970 values. Unilateral absolute values and ratios to the healthy counterparts were evaluated. Visual infarct delineation on each map was also rated. In all spectral maps, the infarct areas could be distinguished from the healthy counterpart by absolute values (p < 0.05). IC, PEN and HA could be distinguished from each other by absolute values (p < 0.05) (except for ED), and by the ratio-value formed to the contralateral side (p < 0.05). Detection of IC and PEN were best possible in ID (IC (AUC = 0.9999, p < 0.0001); PEN (AUC = 0.9745, p < 0.0001)) and MonoE40 (IC (AUC = 0.9963, p < 0.0001); PEN (AUC = 0.9622, p < 0.0001)). Differentiation of IC and PEN was also best in ID (AUC = 0.93, p < 0.0001) and MonoE40 (AUC = 0.80, p < 0.0001). Similarly, visual delineation was best too in ID and MonoE40. Accordingly, IC and PEN can be detected and differentiated in monophasic CTA by using SCT-derived spectral maps like ID or MonoE40.
急性脑卒中成像包括平扫 CT、CT 血管造影(CTA)和 CT 灌注成像(CTP)。CTP 评估不可逆损伤的梗死核心(IC)和有潜力挽救的半暗带(PEN),并将其与健康的实质区域(HA)区分开来。然而,它需要额外的造影剂和辐射。能谱 CT(SCT)可以进行碘密度成像等光谱成像,我们评估了仅使用单相 CTA 数据估计 IC 和 PEN 的潜力。我们分析了 28 例大脑中动脉供血区梗死患者。CTP 分析在梗死侧获得 IC、PEN 和 HA 的区域,以及它们在健康侧的对应区域,并将其作为感兴趣区(ROI)转移到 CTA。光谱测量包括单能量图(MonoE)在 40keV、70keV 和 120keV 下的亨氏单位(HU),以及碘密度(ID)和电子密度(ED)值,共 2970 个值。评估了单侧绝对值和与健康侧对应值的比值。还对每个图谱上的单侧梗死边界进行了评分。在所有光谱图谱中,通过绝对值可以区分梗死区域和健康侧(p<0.05)。通过绝对值(除 ED 外)和与对侧形成的比值可以区分 IC、PEN 和 HA(p<0.05)。在 ID 中可以最好地检测到 IC 和 PEN(IC(AUC=0.9999,p<0.0001);PEN(AUC=0.9745,p<0.0001))和 MonoE40(IC(AUC=0.9963,p<0.0001);PEN(AUC=0.9622,p<0.0001))。在 ID(AUC=0.93,p<0.0001)和 MonoE40(AUC=0.80,p<0.0001)中也可以最好地区分 IC 和 PEN。同样,在 ID 和 MonoE40 中也可以最好地进行视觉边界描绘。因此,通过使用 SCT 衍生的光谱图谱(如 ID 或 MonoE40),可以在单相 CTA 中检测和区分 IC 和 PEN。