Department of Science & Education, Zhengzhou Central Hospital Affiliated to Zhengzhou University, Zhengzhou, PR China.
Department of Radiology, Henan Provincial People's Hospital, Zhengzhou, Henan, China.
PLoS One. 2024 Nov 19;19(11):e0304937. doi: 10.1371/journal.pone.0304937. eCollection 2024.
There is controversy about the benefit of administering adjuvant therapy to esophageal cancer (EC) patients after preoperative neoadjuvant therapy and surgical treatment. This study aims to investigate the clinical benefit of postoperative adjuvant therapy in EC patients with neoadjuvant therapy and surgery.
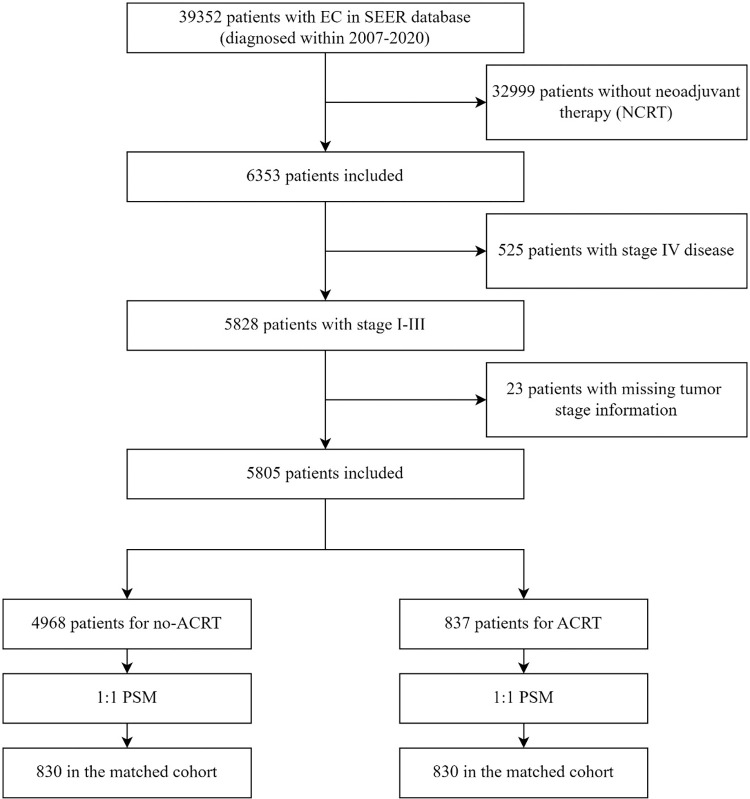
The study included EC patients diagnosed from 2007 to 2020 in the Surveillance, Epidemiology, and End Results (SEER) database. Patients who received neoadjuvant therapy (NCRT) were defined as those who underwent neoadjuvant chemotherapy or neoadjuvant radiotherapy before surgery, while patients who received adjuvant therapy (ACRT) were defined as those who underwent adjuvant chemotherapy or adjuvant radiotherapy after surgery. Propensity score matching (PSM) method was employed to establish matched cohorts, and Kaplan-Meier analysis, COX regression model, and Fine-Gray model were used for survival analysis.
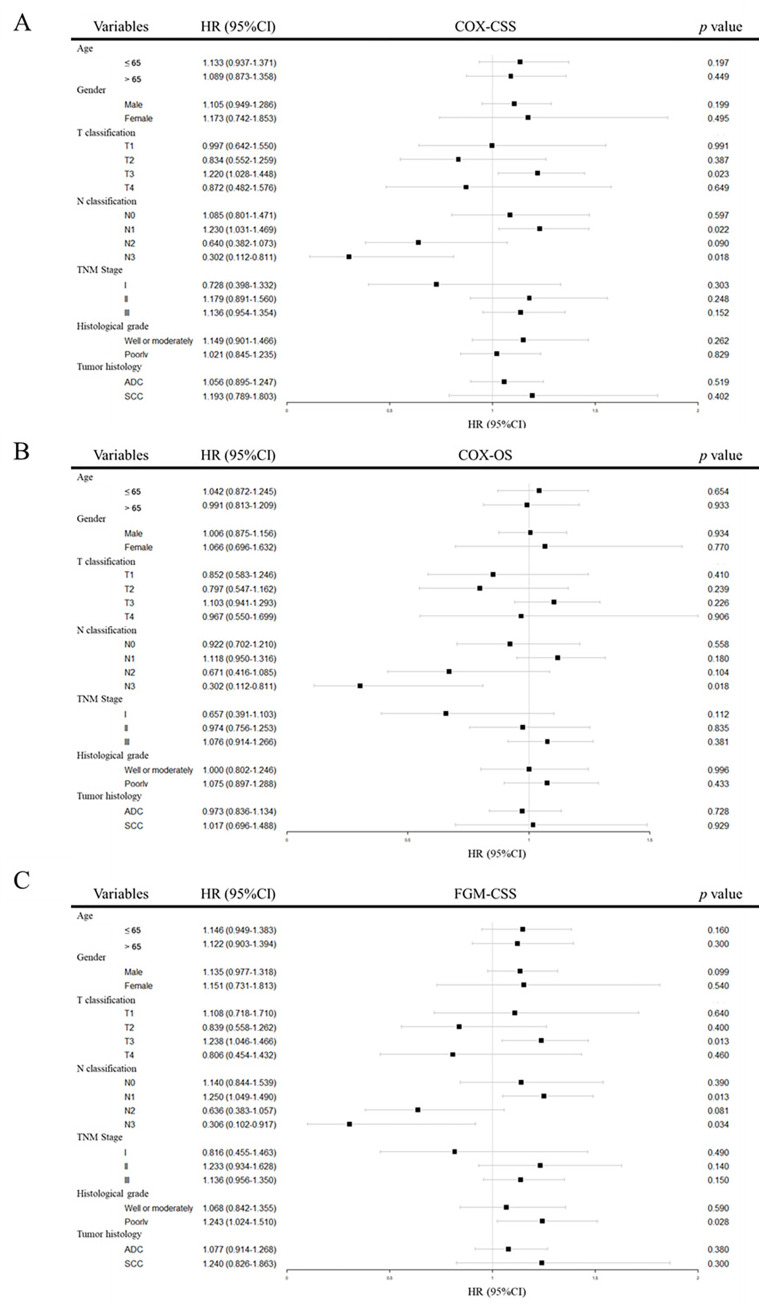
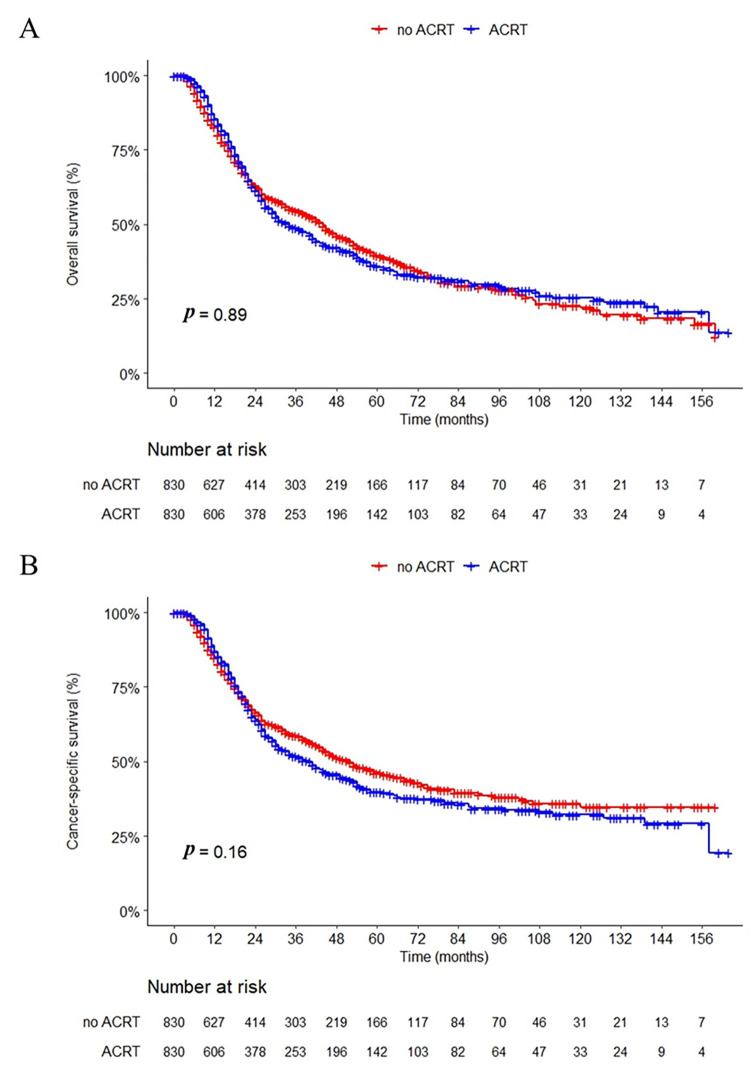
The study included a total of 5805 EC patients, with 837 (14.4%) in the ACRT group and 4968 (85.4%) in the no-ACRT group. After PSM, a cohort of 1660 patients who received NCRT was enrolled for analysis, with 830 patients in each group. Kaplan-Meier analysis revealed no significant differences between the two groups in terms of median overall survival (OS) (34.0 vs. 36.0 months, p = 0.89) or cancer-specific survival (CSS) (40.0 vs. 49.0 months, p = 0.16). Multivariate Cox models and Fine-Gray models indicated that ACRT was not a predictive factor for OS or CSS (p > 0.05). Subgroup analysis for CSS suggested a protective effect of ACRT in the N2 (Cox model: HR = 0.640, p = 0.090; Fine-Gray model: HR = 0.636, p = 0.081) and the N3 subgroup (Cox model: HR = 0.302, p = 0.018; Fine-Gray model: HR = 0.306, p = 0.034).
Only for esophageal cancer patients with a more advanced N stage, postoperative adjuvant therapy after completing neoadjuvant therapy and curative surgical treatment may be beneficial.
术前新辅助治疗和手术治疗后,对食管癌(EC)患者进行辅助治疗的获益存在争议。本研究旨在探讨新辅助治疗和手术治疗后 EC 患者术后辅助治疗的临床获益。
本研究纳入了 2007 年至 2020 年在美国监测、流行病学和最终结果(SEER)数据库中诊断的 EC 患者。接受新辅助治疗(NCRT)的患者定义为接受新辅助化疗或新辅助放疗的患者,而接受辅助治疗(ACRT)的患者定义为接受术后辅助化疗或辅助放疗的患者。采用倾向评分匹配(PSM)方法建立匹配队列,并采用 Kaplan-Meier 分析、COX 回归模型和 Fine-Gray 模型进行生存分析。
本研究共纳入 5805 例 EC 患者,其中 ACRT 组 837 例(14.4%),无 ACRT 组 4968 例(85.6%)。PSM 后,纳入了 1660 例接受 NCRT 的患者进行分析,每组 830 例。Kaplan-Meier 分析显示,两组患者的中位总生存期(OS)(34.0 个月 vs. 36.0 个月,p = 0.89)或癌症特异性生存期(CSS)(40.0 个月 vs. 49.0 个月,p = 0.16)均无显著差异。多变量 Cox 模型和 Fine-Gray 模型表明,ACRT 不是 OS 或 CSS 的预测因素(p > 0.05)。CSS 的亚组分析表明,N2 (Cox 模型:HR = 0.640,p = 0.090;Fine-Gray 模型:HR = 0.636,p = 0.081)和 N3 亚组(Cox 模型:HR = 0.302,p = 0.018;Fine-Gray 模型:HR = 0.306,p = 0.034)中 ACRT 具有保护作用。
只有在新辅助治疗和根治性手术治疗后 N 分期更晚的食管癌患者中,术后辅助治疗可能有益。