Department of Hepatobiliary Surgery, Guangxi Medical University Cancer Hospital, Nanning, 530021, Guangxi Province, China.
Key Laboratory of Early Prevention and Treatment for Regional High Frequency Tumor, Ministry of Education, Nanning, 530021, Guangxi Province, China.
World J Surg Oncol. 2024 Nov 20;22(1):305. doi: 10.1186/s12957-024-03572-6.
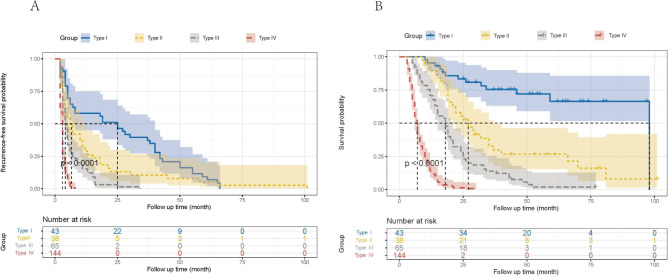
This study aimed to develop postsurgical progression/hyperprogression recurrence (type III-IV recurrence) prediction models for hepatocellular carcinoma (HCC) patients with macroscopic vascular invasion (MaVI) and to guide treatment strategies in the accurate healthcare era.
393 HCC patients with MaVI from two central hospitals made up the entire study population. In developmental (290 patients) and validation (103 patients) cohorts, all patients were randomized into one or the other. Two prediction models for type III-IV recurrence were developed, based on the findings of univariate and multivariate analysis in the development cohort, and multidimensional verification was carried out in both cohorts.
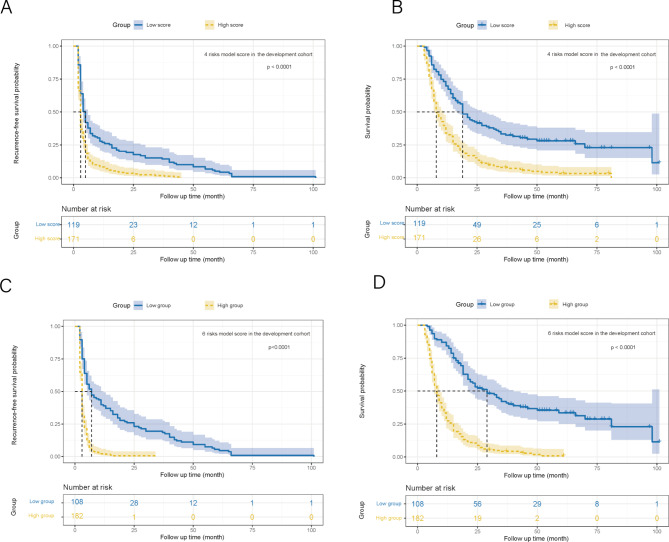
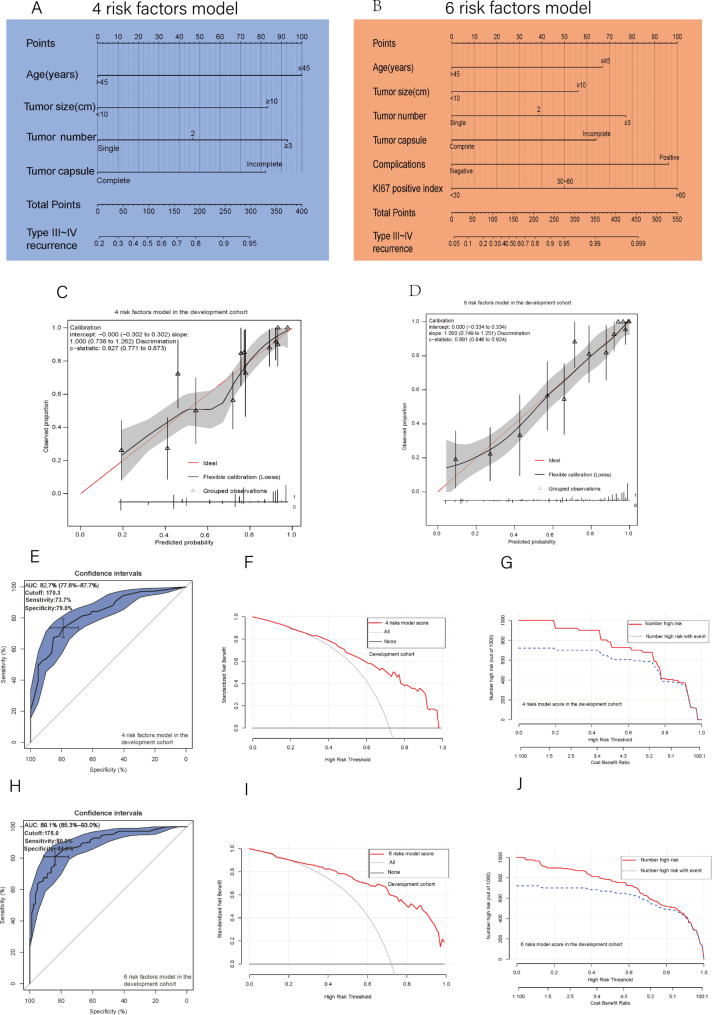
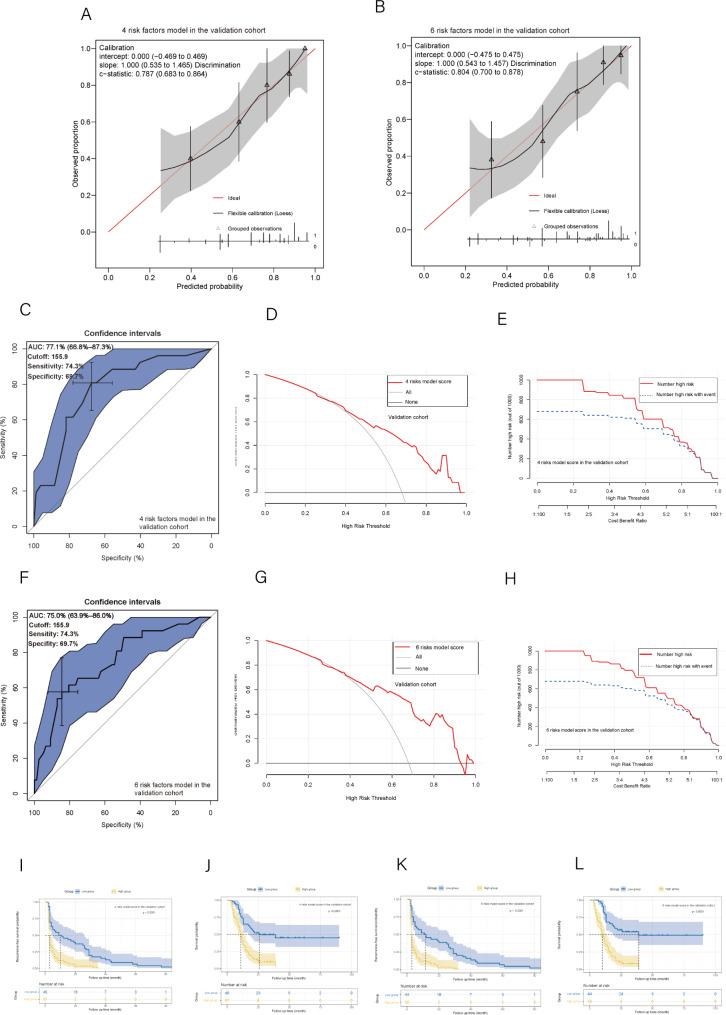
The postoperative recurrence rate of type III-IV in 393 HCC patients with MaVI was 70.9%. Young age, large tumor size (≥ 10 cm), node number, incomplete tumor capsule, postoperative complications, and high Ki67 index were the independent risk factors for relapse of type III-IV. In the development cohort, two nomograms (pre- and postoperative) had the Area Under the ROC curve (AUC) of 0.827 and 0.891, respectively. The two nomograms performed well, according to multidimensional verification methods such as clinical impact curves, decision curve analysis (DCA), and calibration curves. The validation cohort saw similar encouraging results. Both nomograms could separate patients into two distinct prognosis subgroups with ideal cutoff values of 170.3 presurgery and 175.0 postsurgery (both P < 0.05).
We constructed two novel and potentially clinically valuable models for predicting type III-IV recurrence. These two models can develop strategies for treating those suffering from HCC with MaVI owing to their strong prediction performance and availability.
本研究旨在为合并宏观血管侵犯(MaVI)的肝细胞癌(HCC)患者建立术后进展/超进展复发(III-IV 型复发)预测模型,并在精准医疗时代指导治疗策略。
本研究纳入了来自两家中心医院的 393 例合并 MaVI 的 HCC 患者作为研究对象。在开发(290 例)和验证(103 例)队列中,所有患者均被随机分为其中一组。基于开发队列的单因素和多因素分析结果,建立了两种 III-IV 型复发预测模型,并在两个队列中进行了多维验证。
393 例合并 MaVI 的 HCC 患者的术后 III-IV 型复发率为 70.9%。年龄较小、肿瘤较大(≥10cm)、淋巴结数目、肿瘤包膜不完整、术后并发症和 Ki67 指数较高是 III-IV 型复发的独立危险因素。在开发队列中,两种列线图(术前和术后)的 AUC 分别为 0.827 和 0.891。根据临床影响曲线、决策曲线分析(DCA)和校准曲线等多维验证方法,两种列线图均表现良好。验证队列也得到了类似的令人鼓舞的结果。两种列线图均能将患者分为两个不同的预后亚组,术前截点值为 170.3,术后截点值为 175.0(均 P<0.05)。
我们构建了两种用于预测 III-IV 型复发的新型、有潜在临床价值的模型。这两种模型具有较强的预测性能和可用性,可用于制定合并 MaVI 的 HCC 患者的治疗策略。