Intensive Care Unit, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Traditional Chinese Medicine), Hangzhou 310006, Zhejiang Province, China.
World J Gastroenterol. 2024 Nov 14;30(42):4523-4531. doi: 10.3748/wjg.v30.i42.4523.
The prognosis of critically ill patients is closely linked to their gastrointestinal (GI) function. The acute GI injury (AGI) grading system, established in 2012, is extensively utilized to evaluate GI dysfunction and forecast outcomes in clinical settings. In 2021, the GI dysfunction score (GIDS) was developed, building on the AGI grading system, to enhance the accuracy of GI dysfunction severity assessment, improve prognostic predictions, reduce subjectivity, and increase reproducibility.
To compare the predictive capabilities of GIDS and the AGI grading system for 28-day mortality in critically ill patients.
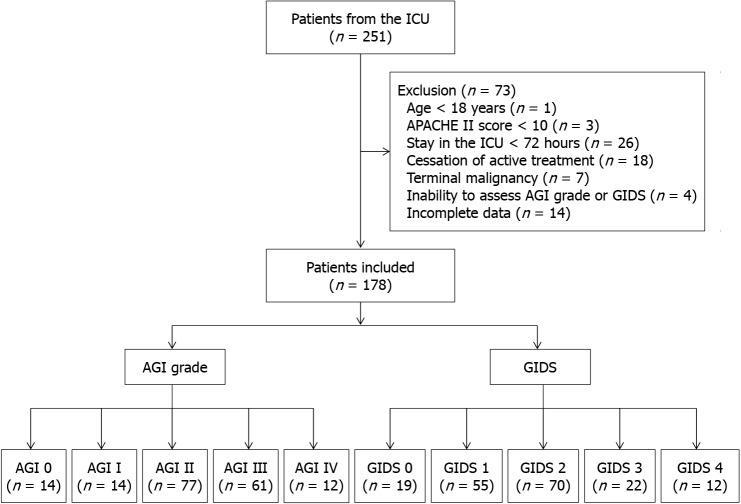
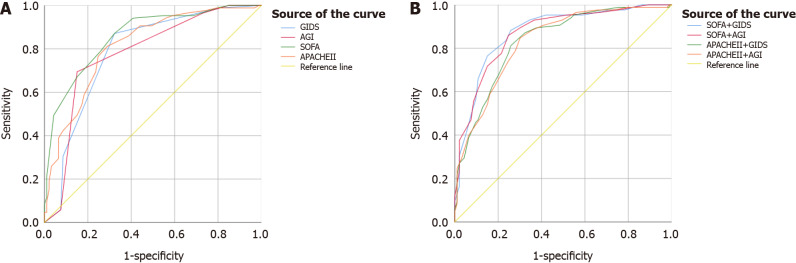
A retrospective study was conducted at the general intensive care unit (ICU) of a regional university hospital. All data were collected during the first week of ICU admission. The primary outcome was 28-day mortality. Multivariable logistic regression analyzed whether GIDS and AGI grade were independent risk factors for 28-day mortality. The predictive abilities of GIDS and AGI grade were compared using the receiver operating characteristic curve, with DeLong's test assessing differences between the curves' areas.
The incidence of AGI in the first week of ICU admission was 92.13%. There were 85 deaths (47.75%) within 28 days of ICU admission. There was no initial 24-hour difference in GIDS between the non-survival and survival groups. Both GIDS (OR 2.01, 95%CI: 1.25-3.24; = 0.004) and AGI grade (OR 1.94, 95%CI: 1.12-3.38; = 0.019) were independent predictors of 28-day mortality. No significant difference was found between the predictive accuracy of GIDS and AGI grade for 28-day mortality during the first week of ICU admission (Z = -0.26, = 0.794).
GIDS within the first 24 hours was an unreliable predictor of 28-day mortality. The predictive accuracy for 28-day mortality from both systems during the first week was comparable.
危重症患者的预后与胃肠道(GI)功能密切相关。2012 年建立的急性胃肠损伤(AGI)分级系统广泛用于评估临床胃肠功能障碍和预测结局。2021 年,基于 AGI 分级系统,开发了胃肠功能障碍评分(GIDS),以提高胃肠功能障碍严重程度评估的准确性,改善预后预测,减少主观性,提高可重复性。
比较 GIDS 和 AGI 分级系统对危重症患者 28 天死亡率的预测能力。
对区域性大学医院综合重症监护病房(ICU)进行回顾性研究。所有数据均在 ICU 入院第一周内收集。主要结局为 28 天死亡率。多变量逻辑回归分析 GIDS 和 AGI 分级是否为 28 天死亡率的独立危险因素。通过受试者工作特征曲线比较 GIDS 和 AGI 分级的预测能力,DeLong 检验评估曲线下面积之间的差异。
ICU 入院第一周 AGI 发生率为 92.13%。ICU 入院后 28 天内死亡 85 例(47.75%)。GIDS 在入住 ICU 后 24 小时内,非存活组与存活组之间无初始差异。GIDS(OR 2.01,95%CI:1.25-3.24;P = 0.004)和 AGI 分级(OR 1.94,95%CI:1.12-3.38;P = 0.019)均为 28 天死亡率的独立预测因子。在 ICU 入院第一周内,GIDS 和 AGI 分级对 28 天死亡率的预测准确性无显著差异(Z = -0.26,P = 0.794)。
入住 ICU 后 24 小时内的 GIDS 是 28 天死亡率的不可靠预测因子。两种系统在 ICU 入院第一周内对 28 天死亡率的预测准确性相当。