Di Giacomo Roberta, Colombo Rachele, Canafoglia Laura, Duran Dunja, Pastori Chiara, Stabile Andrea, Battaglia Giulia, Didato Giuseppe, Cuccarini Valeria, Deleo Francesco, Dominese Ambra, de Curtis Marco, Rossi Sebastiano Davide
Epilepsy Unit, Fondazione IRCCS Istituto Neurologico Carlo Besta, Milan, Italy.
Neuroscience Research Center, Department of Biomedical and Clinical Sciences, University of Milan, Milan, Italy.
Epilepsia. 2025 Jan;66(1):e14-e20. doi: 10.1111/epi.18191. Epub 2024 Nov 22.
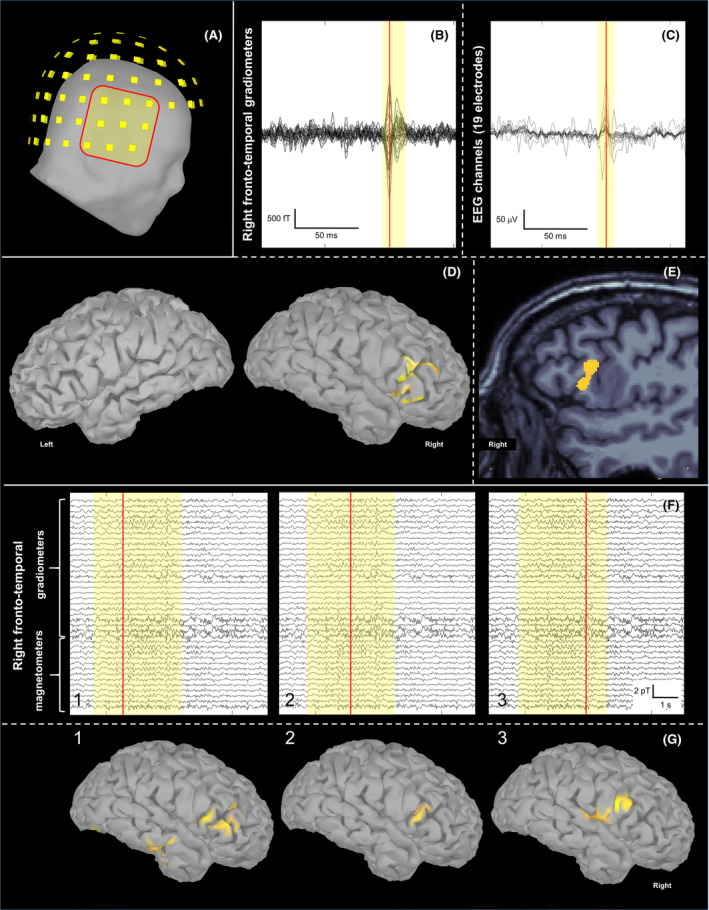
This case report shows the importance of multimodal evaluation to formulate a proper diagnosis of negative motor seizures (NMSs). Only few reports in literature document NMSs with video-electroencephalographic (EEG) and electromyographic coregistration. A multimodal evaluation is crucial to exclude common mimics and propose correct therapy. We describe a case of a 62-year-old man with drug-resistant focal epilepsy and NMSs, evaluated with video-EEG recording with polygraphy, magnetoencephalography (MEG), and brain magnetic resonance imaging (MRI). Video-EEG monitoring showed 182 focal NMSs, with preserved awareness and comprehension. The patient reported complex paresthesia of the left hand followed by left facial grimace, left arm flaccid paralysis, and bradycardia. EEG showed ictal discharges in the right frontocentral region associated with sudden electromyographical silence in left limb muscles consistent with loss of tonic contraction from distal to proximal muscles of the arm. MEG localized the epileptic zone in the right opercular region, consistent with MRI evidence of type II cortical dysplasia in the right inferior frontal gyrus. Multimodal evaluation is essential to document the temporal relationship between ictal discharges, clinical onset of limb paresis, and electrophysiologic evidence of loss of tonic muscular contraction. It allows definition of the specific cortical area involved in NMSs, offering new insight into physiological brain functioning.
本病例报告显示了多模态评估对于准确诊断负性运动性癫痫发作(NMSs)的重要性。文献中仅有少数报告记录了伴有视频脑电图(EEG)和肌电图同步记录的NMSs。多模态评估对于排除常见的模仿症状并提出正确的治疗方法至关重要。我们描述了一例62岁患有耐药性局灶性癫痫和NMSs的男性患者,对其进行了视频脑电图记录并同步记录多导生理数据、脑磁图(MEG)和脑磁共振成像(MRI)评估。视频脑电图监测显示182次局灶性NMSs发作,患者意识和理解能力保留。患者报告左手出现复杂的感觉异常,随后出现左侧面部抽搐、左臂弛缓性麻痹和心动过缓。脑电图显示右侧额中央区发作期放电,同时左侧肢体肌肉突然出现肌电图沉默,这与从手臂远端到近端肌肉的强直性收缩丧失一致。脑磁图将癫痫病灶定位于右侧岛叶区域,这与磁共振成像显示的右侧额下回II型皮质发育异常的证据相符。多模态评估对于记录发作期放电、肢体轻瘫的临床发作以及强直性肌肉收缩丧失的电生理证据之间的时间关系至关重要。它有助于确定参与NMSs的特定皮质区域,为大脑的生理功能提供新的见解。