Princess Máxima Centre for Paediatric Oncology, Utrecht, the Netherlands.
Wilhelmina Children's Hospital, University Medical Centre Utrecht, Utrecht, the Netherlands.
BMC Palliat Care. 2024 Nov 23;23(1):270. doi: 10.1186/s12904-024-01568-3.
In paediatric palliative care, children with life-threatening and life-limiting conditions, their families, and their health care professionals often face difficult decisions about treatment, goals of care, and delivery of care. Advance care planning and shared decision-making are strategies that can improve quality of care by discussing goals and preferences on future care. In this paper, we provide recommendations that aim to optimise advance care planning and shared decision-making in paediatric palliative care in the Netherlands.
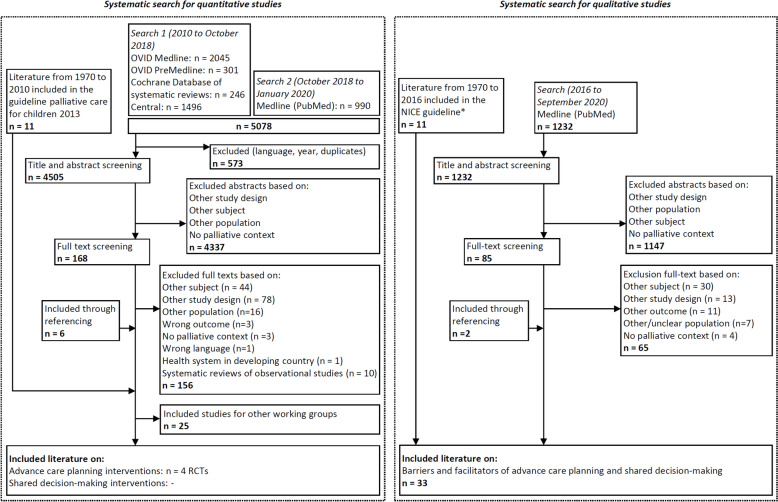
A multidisciplinary guideline panel of 20 experts in paediatric palliative care and nine (bereaved) parents was established to develop recommendations on advance care planning and shared decision-making. We performed systematic literature searches to identify quantitative and qualitative evidence and used the GRADE (CERQual) methodology for appraisal of evidence. Recommendations were formulated based on quantitative and qualitative evidence, clinical expertise, and patient and family experiences.
We identified 4 RCTs that reported on the effect of advance care planning interventions in paediatric palliative care and 33 qualitative studies on barriers and facilitators to advance care planning and shared decision-making. We formulated 28 strong recommendations in close collaboration with a multidisciplinary guideline panel that provide guidance to offer advance care planning and shared decision-making, involve children and their family, and communicate information about care and treatment.
The identified evidence and recommendations support the use of advance care planning and shared decision-making in paediatric palliative care. However, we found several knowledge gaps that should be addressed. As advance care planning and shared decision-making require specific skills and can be time-consuming, we emphasise the importance of education, adequate staffing and sufficient funding to improve integration in clinical practice. We do believe that our recommendations can be used as a starting point to develop recommendations in other countries. However, country-specific factors should be very carefully considered before applying any recommendations in other countries.
在儿科姑息治疗中,患有危及生命和生命有限条件的儿童、他们的家庭以及他们的医疗保健专业人员经常面临关于治疗、护理目标和护理提供的困难决策。预先护理计划和共同决策是通过讨论未来护理的目标和偏好来改善护理质量的策略。在本文中,我们提供了旨在优化荷兰儿科姑息治疗中预先护理计划和共同决策的建议。
成立了一个由 20 名儿科姑息治疗专家和 9 名(已故)父母组成的多学科指南小组,以制定关于预先护理计划和共同决策的建议。我们进行了系统的文献搜索,以确定定量和定性证据,并使用 GRADE(CERQual)方法评估证据。建议是根据定量和定性证据、临床专业知识以及患者和家庭的经验制定的。
我们确定了 4 项 RCT,报告了儿科姑息治疗中预先护理计划干预的效果,以及 33 项关于预先护理计划和共同决策的障碍和促进因素的定性研究。我们与一个多学科指南小组密切合作制定了 28 项强有力的建议,为提供预先护理计划和共同决策、涉及儿童及其家庭以及沟通护理和治疗信息提供了指导。
确定的证据和建议支持在儿科姑息治疗中使用预先护理计划和共同决策。然而,我们发现了几个知识空白,应该加以解决。由于预先护理计划和共同决策需要特定的技能并且可能很耗时,因此我们强调教育、充足的人员配备和足够的资金的重要性,以改善在临床实践中的整合。我们确实相信,我们的建议可以作为制定其他国家建议的起点。然而,在将任何建议应用于其他国家之前,应非常仔细地考虑国家特定因素。