Department of Obstetrics and Gynecology, Sun Yat-Sen Memorial Hospital of Sun Yat-Sen University, Yuexiu District, No.107 Yanjiang West Road, Guangzhou, 510120, China.
Guangdong Provincial Clinical Research Center for Obstetrical and Gynecological Diseases, Guangzhou, China.
BMC Womens Health. 2024 Nov 22;24(1):619. doi: 10.1186/s12905-024-03457-6.
Conservative surgery for adenomyosis has been shown to be effective. However, risk factors for postoperative recurrence have yet to be clarified. In this study, we aimed to determine the recurrence rate after conservative surgery for adenomyosis and identify the risk factors for recurrence.
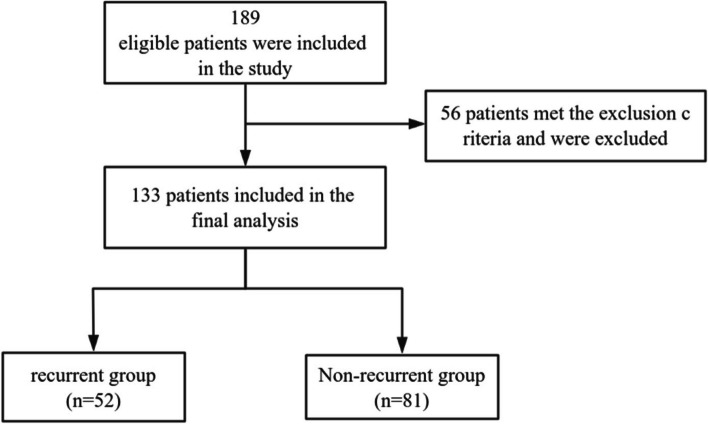
This retrospective study was conducted in a tertiary hospital. Patients who underwent conservative surgery for adenomyosis between January 2013 and April 2023 were identified. Eligible patients were assigned to either the recurrent or non-recurrent group. Continuous and categorical variables were compared between the two groups using the Mann-Whitney U test or chi-squared test. Risk factors for recurrence were identified by Cox proportional risk analysis.
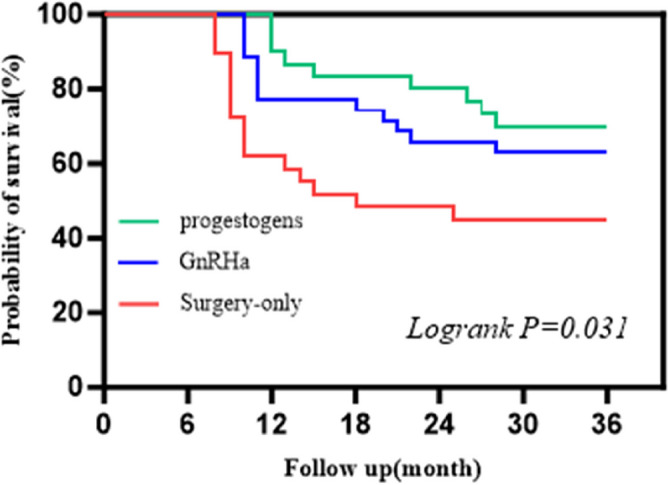
Data for 133 eligible patients who underwent conservative surgery for adenomyosis were analyzed. The mean follow-up duration was 52 months. The recurrence rate after conservative surgery was 39.1% (52/133). Cox proportional risk analysis identified adenomyosis involving the posterior uterine wall (hazard ratio [HR] 6.505, P = 0.018), two or more adenomyotic lesions (HR 6.310, P = 0.030), laparotomy (HR 2.490, P = 0.029), and concomitant endometriosis (HR 2.313, P = 0.036) to be risk factors for recurrence after conservative surgery. Postoperative combined progestogen therapy (HR 0.126, P < 0.001) or treatment with a gonadotropin-releasing hormone agonist (GnRHa) (HR 0.237, P = 0.004) prevented recurrence of adenomyosis.
Adenomyosis continues to have a relatively high long-term recurrence rate after conservative surgery. Patients with adenomyosis involving the posterior wall of the uterus, those with two or more adenomyotic lesions, and those with concomitant endometriosis are at high risk for recurrence after conservative surgery. Postoperative progestogen or GnRHa therapy may reduce the risk of recurrence of adenomyosis. Considering the retrospective nature of this study and its small sample size, larger prospective studies are needed to confirm its findings.
保守手术治疗子宫腺肌病已被证明是有效的。然而,术后复发的风险因素仍未阐明。本研究旨在确定子宫腺肌病保守手术后的复发率,并确定复发的风险因素。
这是一项在一家三级医院进行的回顾性研究。确定了 2013 年 1 月至 2023 年 4 月期间接受子宫腺肌病保守手术的患者。符合条件的患者被分配到复发或非复发组。连续和分类变量使用 Mann-Whitney U 检验或卡方检验进行比较。使用 Cox 比例风险分析确定复发的风险因素。
对 133 名接受子宫腺肌病保守手术的患者进行了数据分析。平均随访时间为 52 个月。保守手术后的复发率为 39.1%(52/133)。Cox 比例风险分析确定了子宫腺肌病累及子宫后壁(风险比 [HR] 6.505,P=0.018)、两个或更多的腺肌病病灶(HR 6.310,P=0.030)、剖腹手术(HR 2.490,P=0.029)和同时存在子宫内膜异位症(HR 2.313,P=0.036)是保守手术后复发的风险因素。术后联合孕激素治疗(HR 0.126,P<0.001)或使用促性腺激素释放激素激动剂(GnRHa)治疗(HR 0.237,P=0.004)可预防子宫腺肌病的复发。
子宫腺肌病在保守手术后仍有相对较高的长期复发率。累及子宫后壁的子宫腺肌病、有两个或更多腺肌病病灶的患者以及同时存在子宫内膜异位症的患者,保守手术后复发的风险较高。术后孕激素或 GnRHa 治疗可能降低子宫腺肌病复发的风险。考虑到本研究的回顾性性质和样本量较小,需要更大规模的前瞻性研究来证实其发现。