Reinier Haga Orthopedic Center, Zoetermeer, The Netherlands.
Department of Orthopaedics and Sports Medicine, Erasmus MC, University Medical Center Rotterdam, Rotterdam, The Netherlands.
Syst Rev. 2024 Nov 22;13(1):286. doi: 10.1186/s13643-024-02694-y.
While shared decision making is a cornerstone of orthopedic care, orthopedic surgeons face challenges in tailoring their advice and expectation management to individual shoulder arthroplasty patients due to the lack of systematically summarized evidence-based knowledge. This systematic review aims to provide an overview of current knowledge on independent predictive effects of patient-related factors on functional and pain-related outcomes after shoulder arthroplasty.
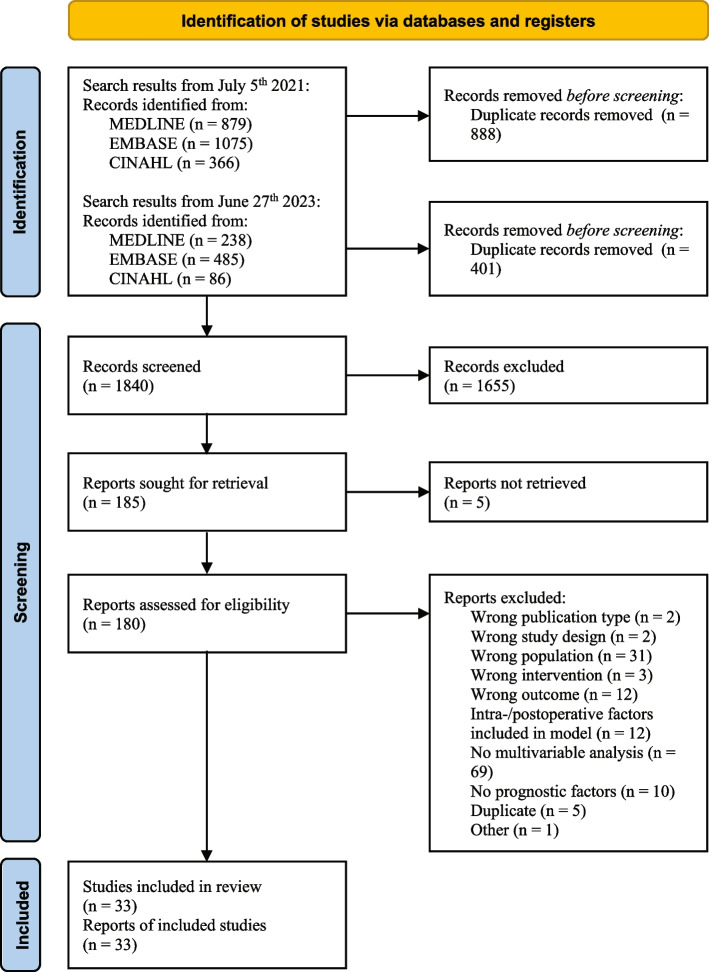
We included longitudinal cohort studies including patients receiving total or reverse shoulder arthroplasty or hemiarthroplasty for primary osteoarthritis or cuff tear arthropathy. Studies with only univariable analyses were excluded. MEDLINE, Embase, and CINAHL databases were last searched on June 27, 2023. Risk of bias was evaluated using the QUIPS tool. For the analyses, we divided outcomes into three domains (Functional Recovery, Pain, and Functional Recovery & Pain) and four time points (short term, medium-short term, medium-long term and long term). When appropriate, meta-analyses were conducted to pool regression coefficients or odds ratios. Otherwise, results were summarized in a qualitative analysis. We used the GRADE approach to rate the certainty of the evidence.
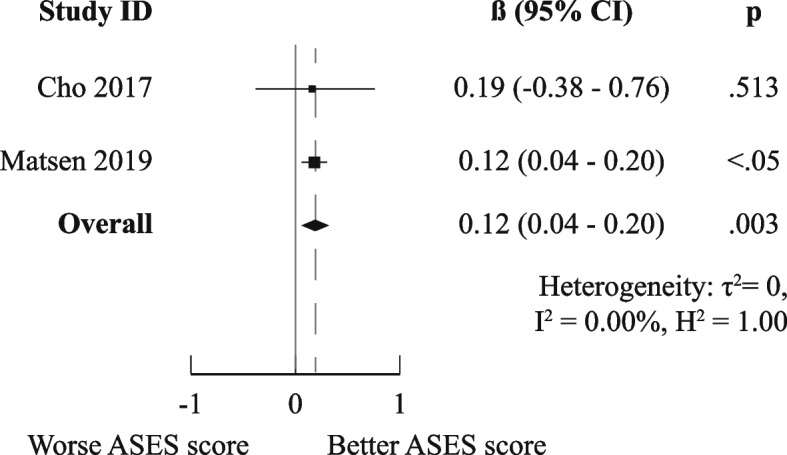
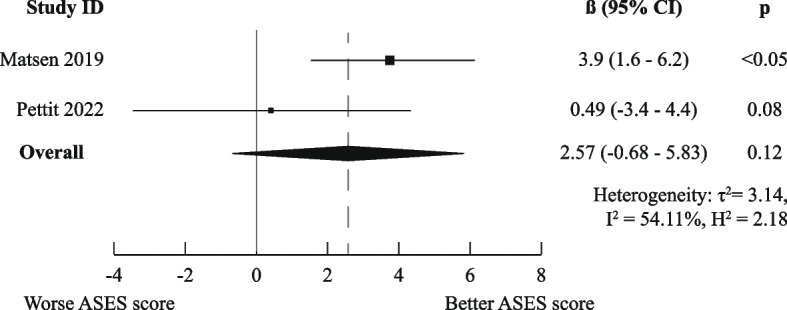
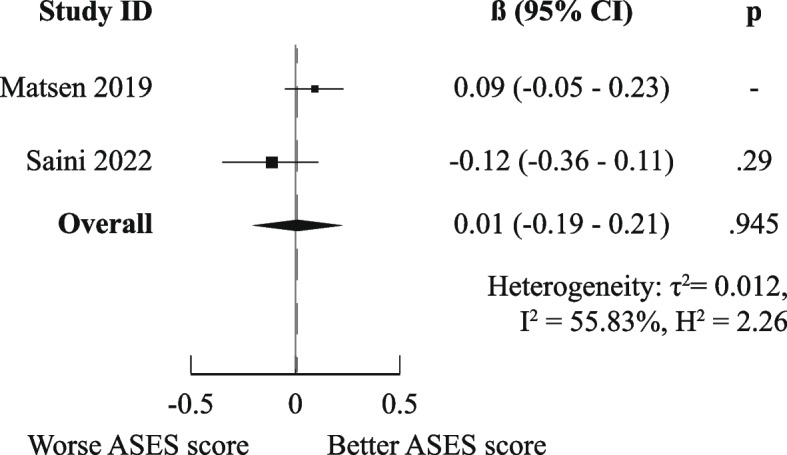
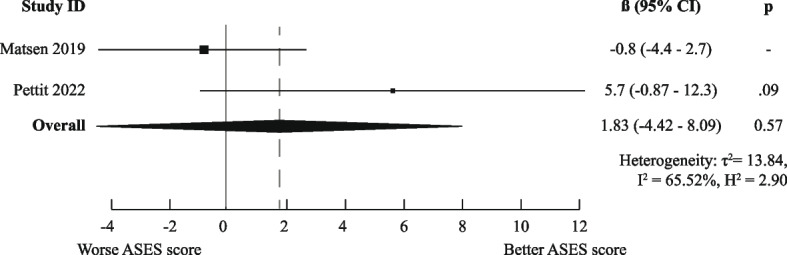
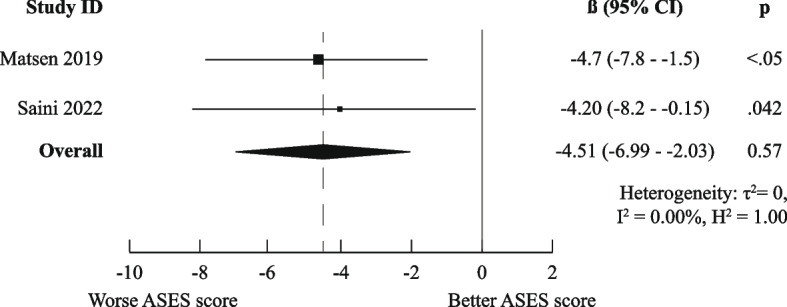
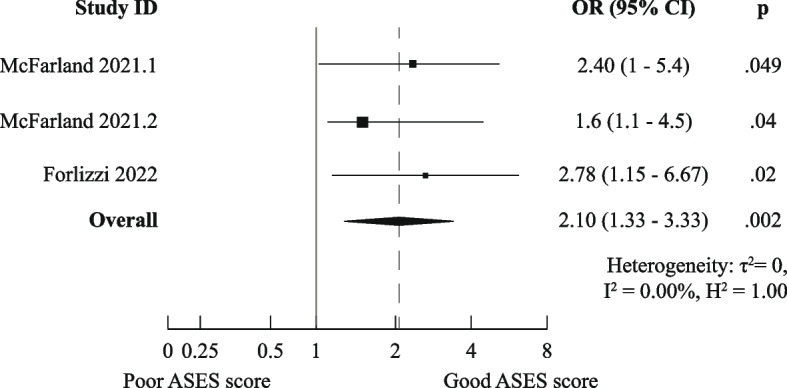
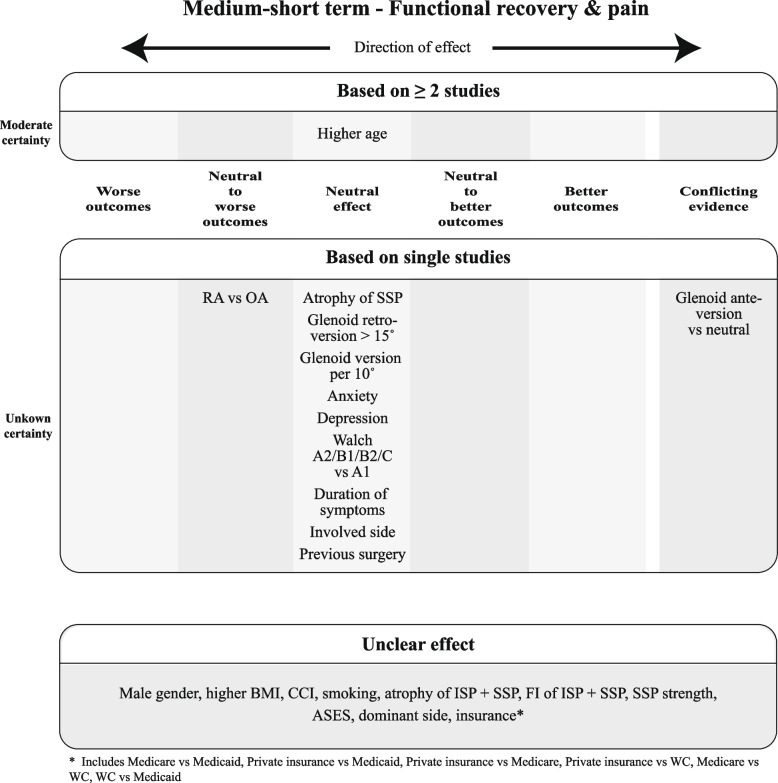
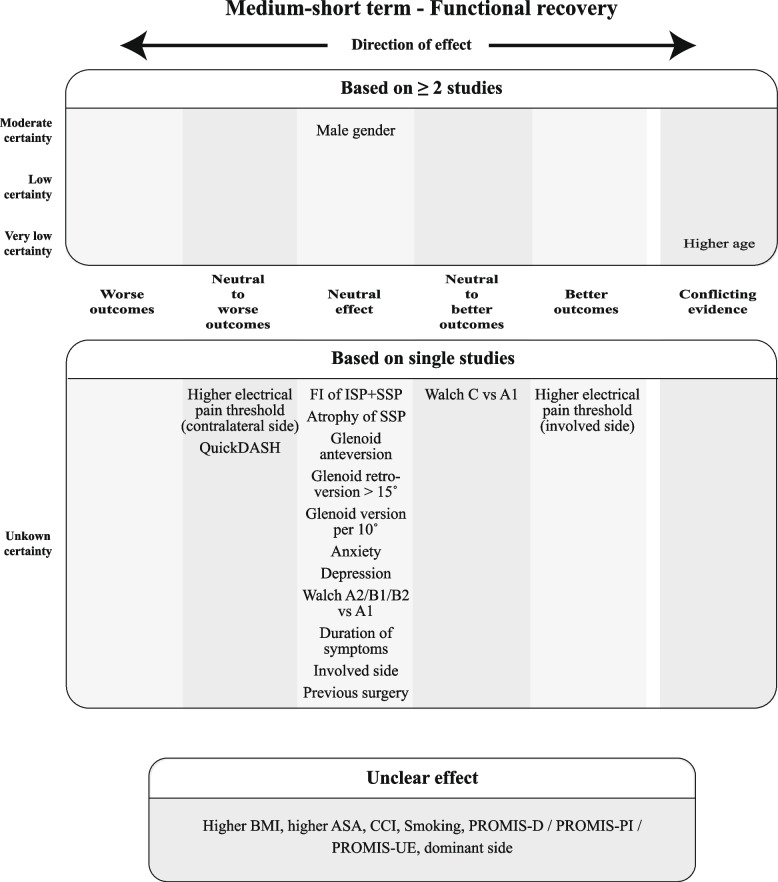
Thirty-three studies analyzing over 6900 patients were included; these studied 16 PROMs and 52 prognostic factors. We could perform meta-analyses for six combinations of prognostic factor, domain, and time point. Only the meta-analysis for medium-long term poor ASES scores indicated worse outcomes for previous shoulder surgery (OR (95%CI) of 2.10 (1.33-3.33)). The majority of reported factors showed unclear or neutral independent effects on functional outcomes.
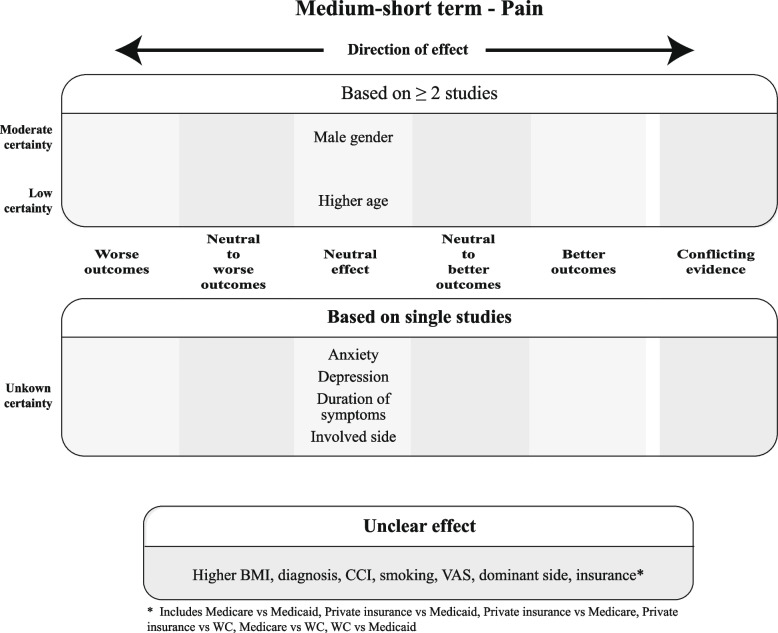
Methodological heterogeneity and selective/incomplete reporting prevented us from pooling most results, culminating in a largely qualitative analysis. Depression, preoperative opioid use, preoperative ASES and SST scores, surgery on the dominant side, previous surgery, male gender, no. of patient-reported allergies, back pain, living alone, CTA vs OA, diabetes, and greater preoperative external ROM predicted neutral to worse or worse outcomes. In contrast, higher electrical pain threshold on the operative side, OA/RCA vs other diagnosis, and private insurance vs Medicaid/Medicare predicted neutral to better or better outcomes. These results can help orthopedic surgeons tailor their advice and better manage expectations.
PROSPERO CRD42021284822.
尽管共同决策是骨科护理的基石,但由于缺乏系统总结的循证知识,骨科医生在为每位肩关节置换患者提供建议和管理期望方面面临挑战。本系统评价旨在概述患者相关因素对肩关节置换后功能和疼痛相关结局的独立预测影响的现有知识。
我们纳入了包括接受全肩关节置换、反肩关节置换或半肩关节置换治疗原发性骨关节炎或肩袖撕裂性关节炎的患者的纵向队列研究。排除仅进行单变量分析的研究。最后一次检索 MEDLINE、Embase 和 CINAHL 数据库是在 2023 年 6 月 27 日。使用 QUIPS 工具评估偏倚风险。对于分析,我们将结局分为三个领域(功能恢复、疼痛和功能恢复与疼痛)和四个时间点(短期、中短期、中长期和长期)。在适当的情况下,进行荟萃分析以汇总回归系数或优势比。否则,结果以定性分析进行总结。我们使用 GRADE 方法对证据的确定性进行评级。
纳入了 33 项分析了超过 6900 名患者的研究;这些研究了 16 项 PROMs 和 52 个预后因素。我们可以对六个预后因素、领域和时间点的组合进行荟萃分析。只有中长期 ASES 评分较差的荟萃分析表明先前的肩部手术结果较差(OR(95%CI)为 2.10(1.33-3.33))。报告的大多数因素对功能结局的独立影响不明确或中性。
方法学异质性和选择性/不完整报告阻止了我们对大多数结果进行汇总,最终导致了主要是定性分析。抑郁、术前阿片类药物使用、术前 ASES 和 SST 评分、优势侧手术、既往手术、男性、患者报告的过敏次数、背痛、独居、肩袖撕裂性关节炎与其他诊断、糖尿病、术前外展ROM 更大预测结果为中性至更差或更差。相比之下,术侧电痛阈更高、肩袖撕裂性关节炎与其他诊断、私人保险优于医疗补助/医疗保险预测结果为中性至更好或更好。这些结果可以帮助骨科医生为每位患者提供建议并更好地管理预期。
PROSPERO CRD42021284822。