From the Department of Pediatric Infectious Diseases, Institute of Tropical Medicine (L.-M.Y., M. Toizumi, C.I., M. Takegata), the Department of Global Health, School of Tropical Medicine and Global Health (L.-M.Y., M. Toizumi), and Nagasaki University Graduate School of Biomedical Science (L.-M.Y.), Nagasaki University, Nagasaki, and the National Institute of Infectious Diseases, Tokyo (N.K.) - both in Japan; the Department of Bacteriology, National Institute of Hygiene and Epidemiology, Hanoi (H.A.T.N., L.H.H., D.-A.D.), and the Department of Bacteriology, Pasteur Institute, Nha Trang (L.T.L., H.T.D.) - both in Vietnam; the Department of Infectious Disease Epidemiology (B.J.Q., K.Z., K.M., S.F.) and the Centre for Mathematical Modelling of Infectious Diseases (B.J.Q., K.Z., S.F.), London School of Hygiene and Tropical Medicine, and the Institute for Infection and Immunity, St. George's University (J.H.) - both in London; the Department of Infection, Immunity, and Global Health, Murdoch Children's Research Institute (M.L.N., B.D.O., E.M.D., C.S., K.M.), and the Department of Paediatrics, University of Melbourne (C.S., K.M.), Melbourne, VIC, and the Department of Microbiology and Immunology, Peter Doherty Institute for Infection and Immunity, University of Melbourne, Parkville, VIC (C.S.) - all in Australia; and the Center for Global Health, Charité-Universitätmedizin Berlin, Berlin (S.F.).
N Engl J Med. 2024 Nov 28;391(21):1992-2002. doi: 10.1056/NEJMoa2400007.
After pneumococcal disease and colonization have been controlled through vaccination campaigns, a reduced pneumococcal conjugate vaccine (PCV) schedule may be sufficient to sustain that control at reduced costs.
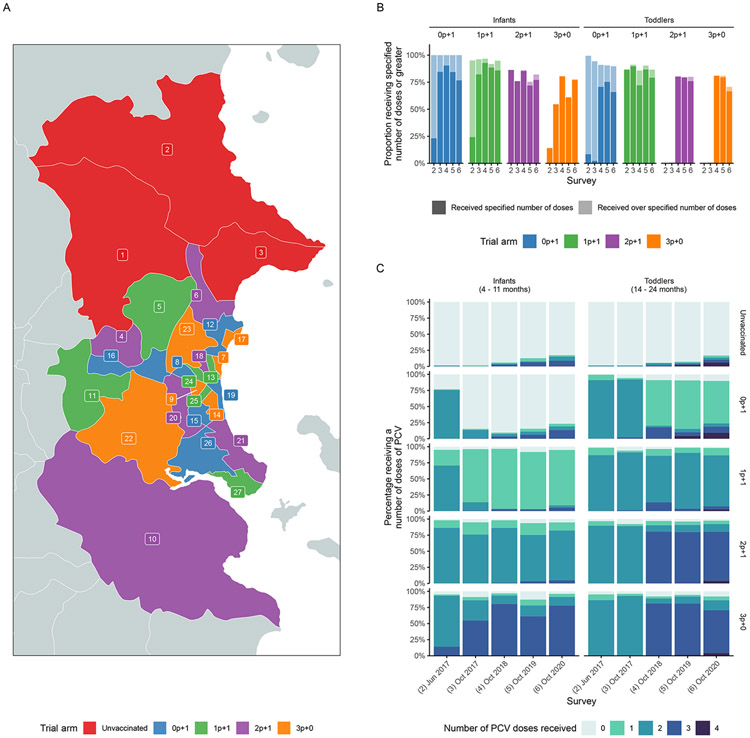
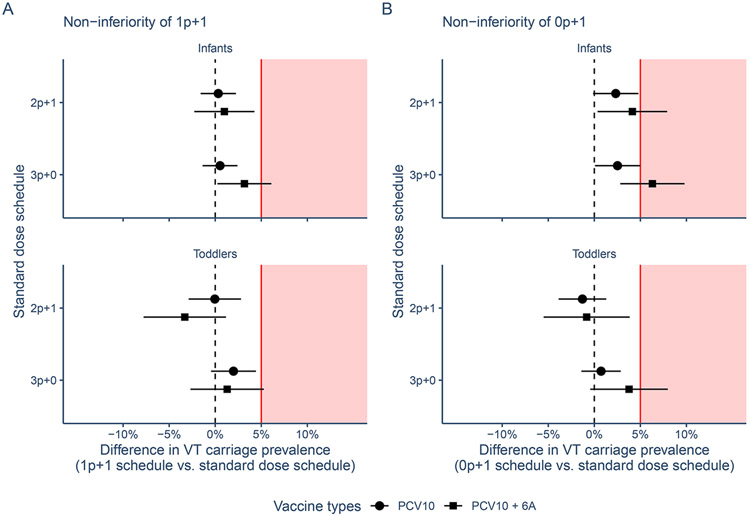
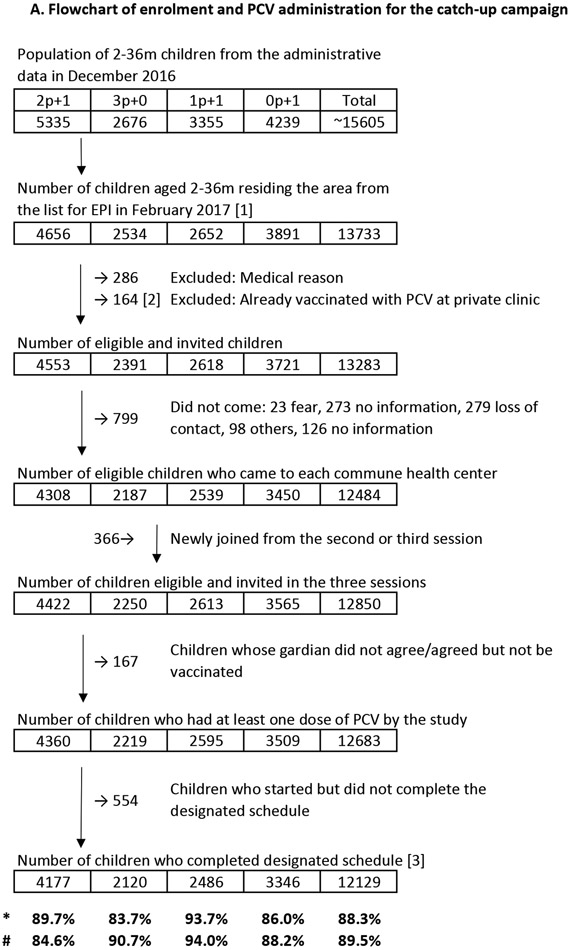
We investigated whether a single primary dose and booster dose (1p+1) of the 10-valent PCV (PCV10) would be noninferior to alternative dose schedules in sustaining control of carriage of pneumococcal serotypes included in the vaccine. In Nha Trang, Vietnam, an area in which PCV had not been used previously, a PCV10 catch-up campaign was conducted in which the vaccine was offered to children younger than 3 years of age, after which a cluster-randomized trial was conducted in which children received PCV10 at 2, 3, and 4 months of age (3p+0 group); at 2, 4, and 12 months of age (2p+1 group); at 2 and 12 months of age (1p+1 group); or at 12 months of age (0p+1 group). Annual carriage surveys in infants (4 to 11 months of age) and toddlers (14 to 24 months of age) were conducted from 2016 through 2020. The primary end point was protection against carriage of vaccine serotypes, evaluated in a noninferiority analysis in the 1p+1 group as compared with the 2p+1 and 3p+0 groups, 3.5 years after vaccine introduction (noninferiority margin, 5 percentage points). Noninferiority of the 0p+1 schedule was also evaluated.
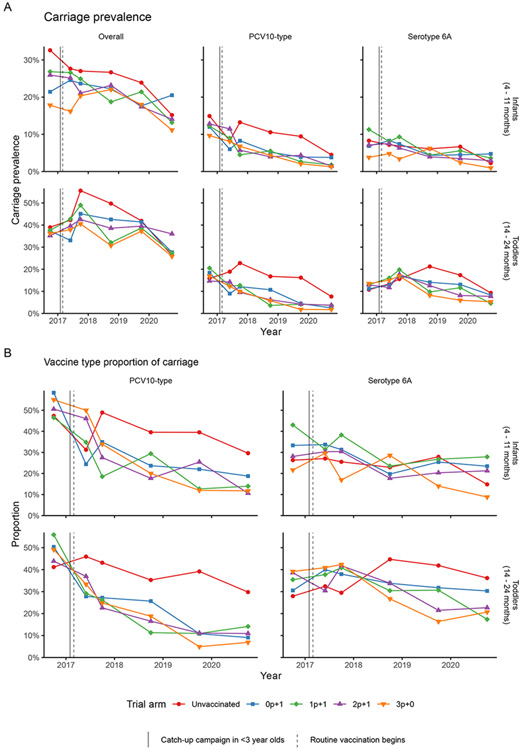
In 2016, before the introduction of PCV10, vaccine-serotype carriage was found in 160 of 1363 infants (11.7%); in 2020, vaccine-serotype carriage was found in 6 of 333 (1.8%), 5 of 340 (1.5%), and 4 of 313 (1.3%) infants in the 1p+1, 2p+1, and 3p+0 groups, respectively, indicating noninferiority of 1p+1 to 2p+1 (difference, 0.3 percentage points; 95% confidence interval [CI], -1.6 to 2.2) and to 3p+0 (difference, 0.5 percentage points; 95% CI, -1.4 to 2.4). Similarly, 1p+1 was noninferior to 2p+1 and 3p+0 for protection against vaccine-serotype carriage among toddlers. In 2016, carriage of serotype 6A was found in 99 of 1363 infants (7.3%); in 2020, it was found in 12 of 333 (3.6%), 10 of 340 (2.9%), and 3 of 313 (1.0%) infants in the 1p+1, 2p+1, and 3p+0 groups, respectively. The 0p+1 schedule was also noninferior to the other three dose schedules among infants and toddlers, although cross-protection against serotype 6A was less common than with the other vaccination schedules. No PCV10-associated severe adverse effects were observed.
A reduced vaccination schedule involving a single primary dose and booster dose of PCV10 was noninferior to alternative schedules in protecting against vaccine-serotype carriage in infants and toddlers. (Funded by the Bill and Melinda Gates Foundation and others; ClinicalTrials.gov number, NCT02961231.).
在通过疫苗接种运动控制了肺炎球菌疾病和定植后,减少的肺炎球菌结合疫苗(PCV)方案可能足以在降低成本的情况下维持这种控制。
我们研究了 10 价 PCV(PCV10)的单次基础剂量和加强剂量(1p+1)是否在维持疫苗涵盖的血清型携带的控制方面不劣于替代剂量方案。在越南芽庄,这是一个以前没有使用过 PCV 的地区,进行了一次 PCV10 补种运动,为 3 岁以下的儿童提供疫苗,之后在一个群组随机试验中,儿童在 2、3 和 4 个月龄时(3p+0 组);在 2、4 和 12 个月龄时(2p+1 组);在 2 和 12 个月龄时(1p+1 组);或在 12 个月龄时(0p+1 组)接种 PCV10。从 2016 年到 2020 年,每年对婴儿(4 至 11 个月龄)和幼儿(14 至 24 个月龄)进行携带调查。主要终点是在疫苗引入后 3.5 年,评估 1p+1 组相对于 2p+1 和 3p+0 组对疫苗血清型携带的保护作用,非劣效性分析的非劣效性边界为 5 个百分点。还评估了 0p+1 方案的非劣效性。
2016 年,在引入 PCV10 之前,在 1363 名婴儿中有 160 名(11.7%)发现了疫苗血清型携带;2020 年,在 1p+1、2p+1 和 3p+0 组中,分别有 6/333(1.8%)、5/340(1.5%)和 4/313(1.3%)婴儿发现疫苗血清型携带,表明 1p+1 与 2p+1(差异,0.3 个百分点;95%置信区间 [CI],-1.6 至 2.2)和 3p+0(差异,0.5 个百分点;95%CI,-1.4 至 2.4)的非劣效性。同样,1p+1 在幼儿中对疫苗血清型携带的保护作用也不劣于 2p+1 和 3p+0。2016 年,在 1363 名婴儿中有 99 名(7.3%)发现血清型 6A 携带;在 2020 年,在 1p+1、2p+1 和 3p+0 组中,分别有 12/333(3.6%)、10/340(2.9%)和 3/313(1.0%)婴儿发现血清型 6A 携带。0p+1 方案在婴儿和幼儿中也不劣于其他三种剂量方案,尽管与其他疫苗接种方案相比,对血清型 6A 的交叉保护作用较少。没有观察到与 PCV10 相关的严重不良事件。
减少的包含单次基础剂量和加强剂量的 PCV10 疫苗接种方案在预防婴儿和幼儿疫苗血清型携带方面不劣于替代方案。(由比尔及梅琳达·盖茨基金会等资助;ClinicalTrials.gov 编号,NCT02961231。)