Department of Urology, Urology Research Institute, the First Affiliated Hospital, Fujian Medical University, Fuzhou, 350005, China.
Department of Urology, Binhai Campus of the First Affiliated Hospital, National Region Medical centre, Fujian Medical University, Fuzhou, 350212, China.
BMC Cancer. 2024 Nov 27;24(1):1459. doi: 10.1186/s12885-024-13207-4.
To build and validate a periprostatic fat magnetic resonance imaging (MRI) based radiomics nomogram for prediction of biochemical recurrence-free survival (bRFS) of patients with non-metastatic prostate cancer (PCa) receiving radical prostatectomy (RP).
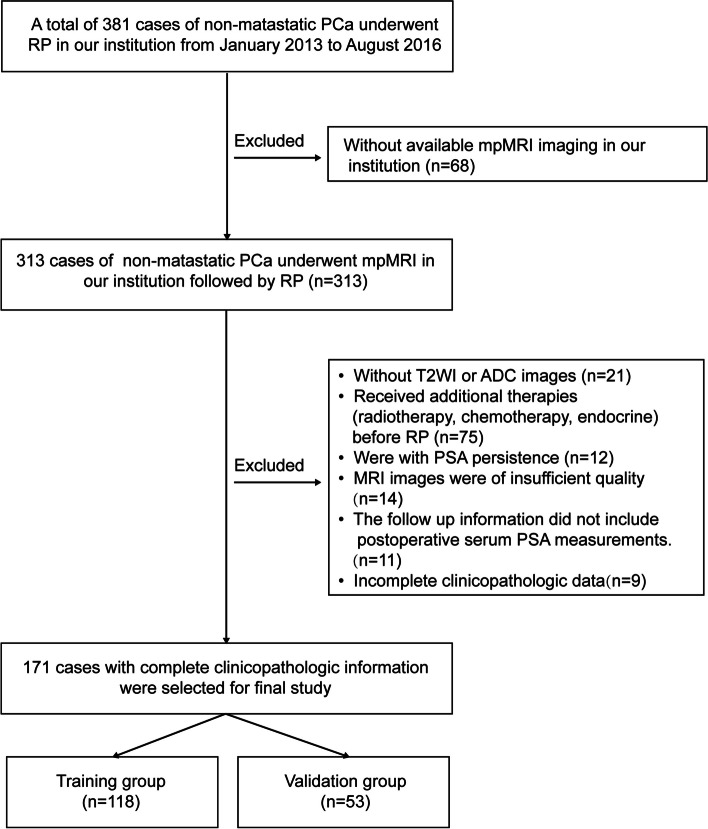
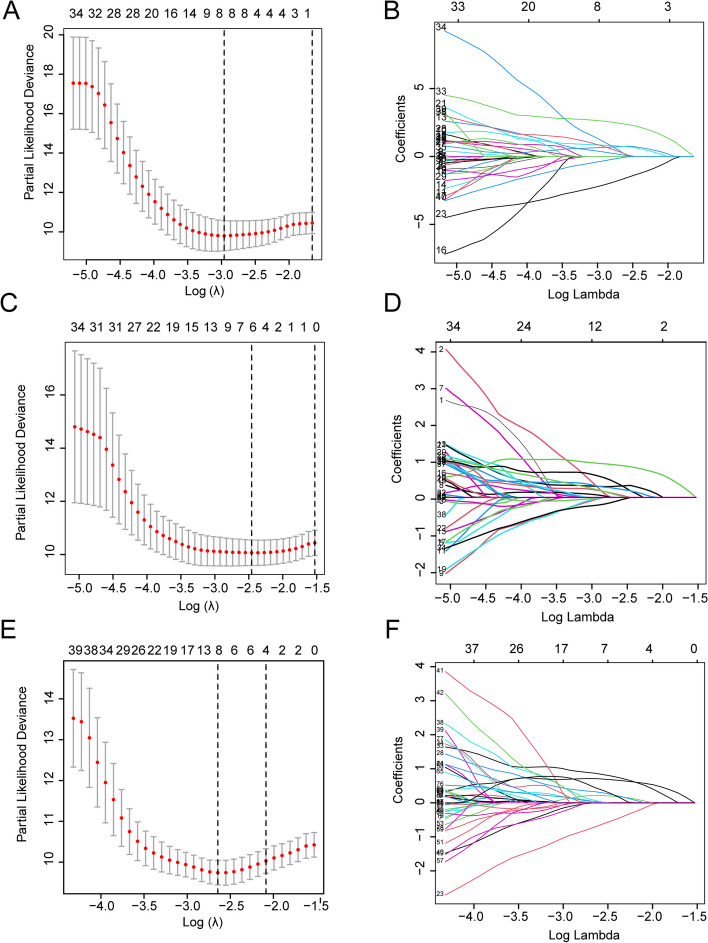
A retrospective study was conducted on 356 patients with non-metastatic PCa who underwent preoperative mpMRI followed by RP treatment at our institution. Radiomic features were extracted from both intratumoral region and the periprostatic fat region, which were segmented on images obtained through T2-weighted imaging (T2WI) and apparent-diffusion coefficient (ADC) imaging. Three radiomics models were developed by applying the Least absolute shrinkage and selection operator (LASSO) Cox regression, followed by Cox risk regression to construct a combined radiomics-clinical model by integrating the optimal radiomics score and clinicopathological risk factors to draw a nomogram. The predictive performance was evaluated using receiver operating characteristic (ROC) curves, Kaplan-Meier analysis and calibration curves.
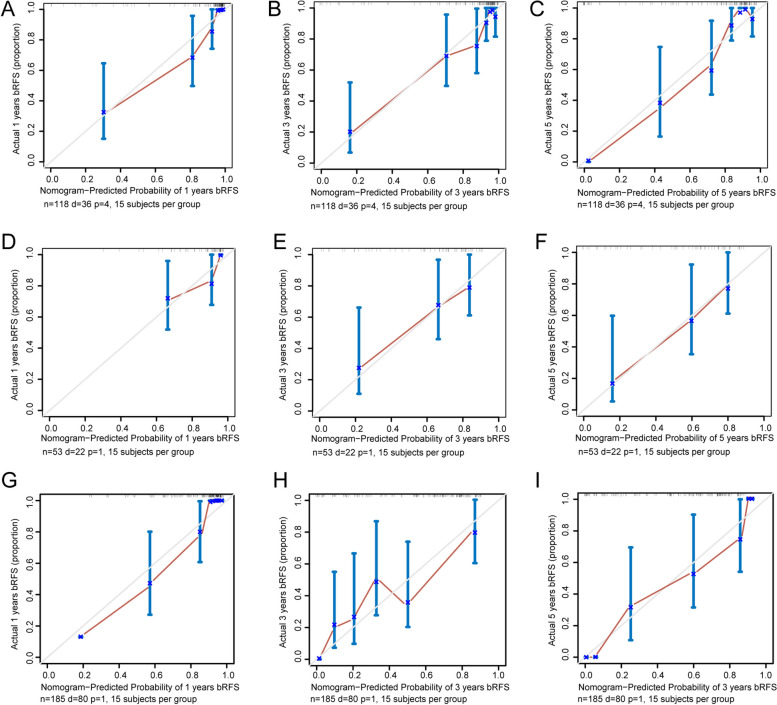
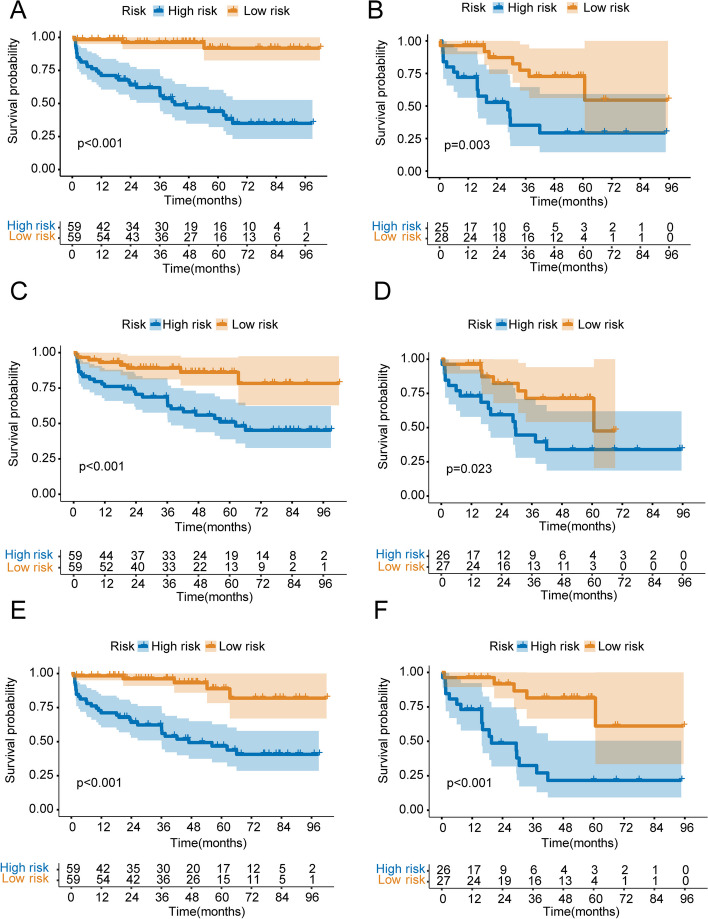
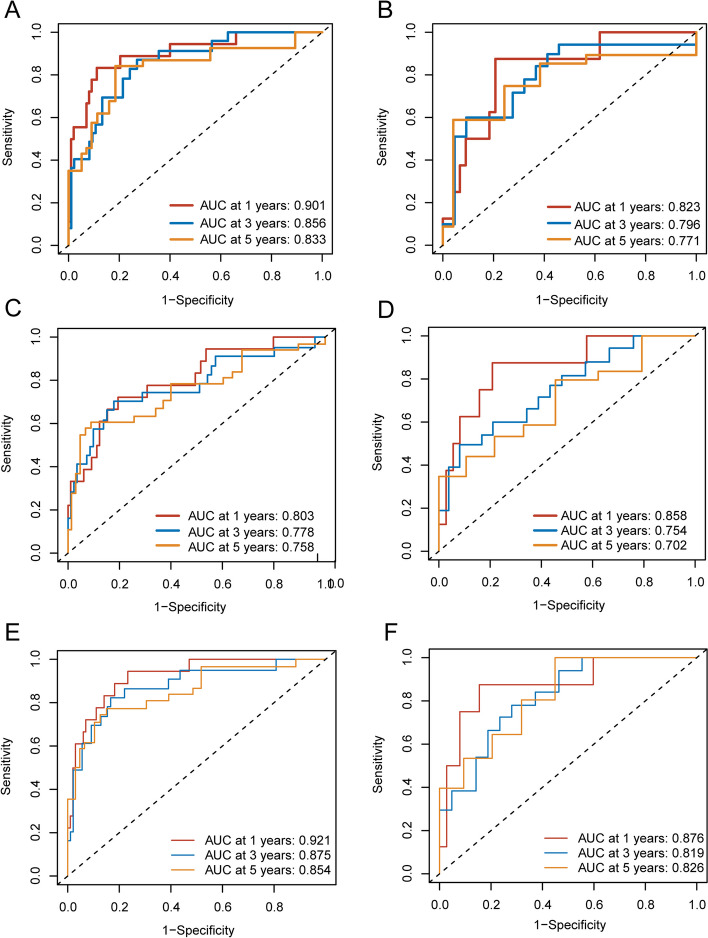
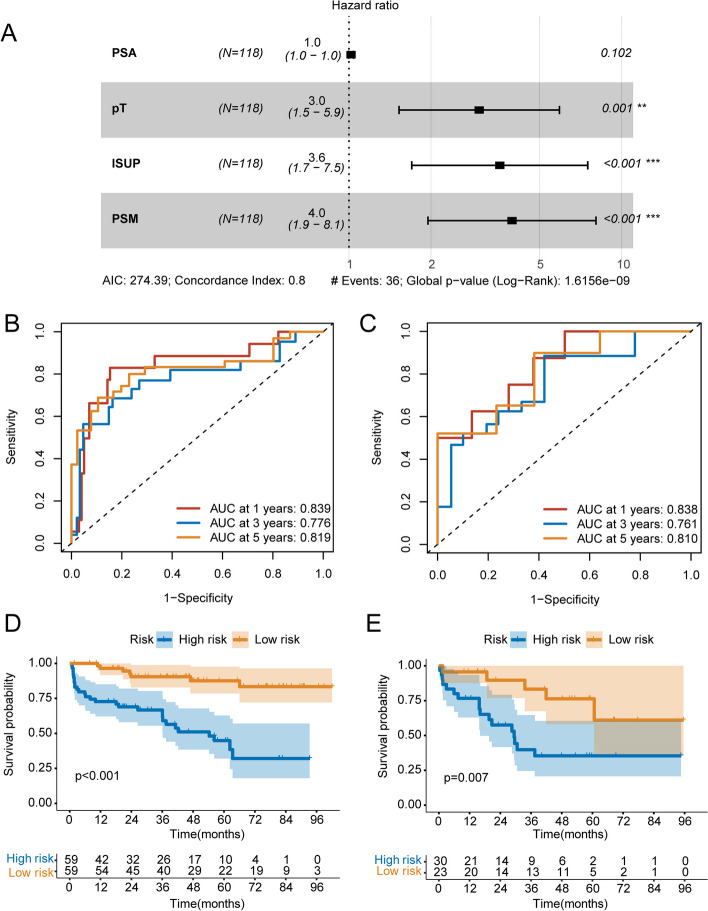
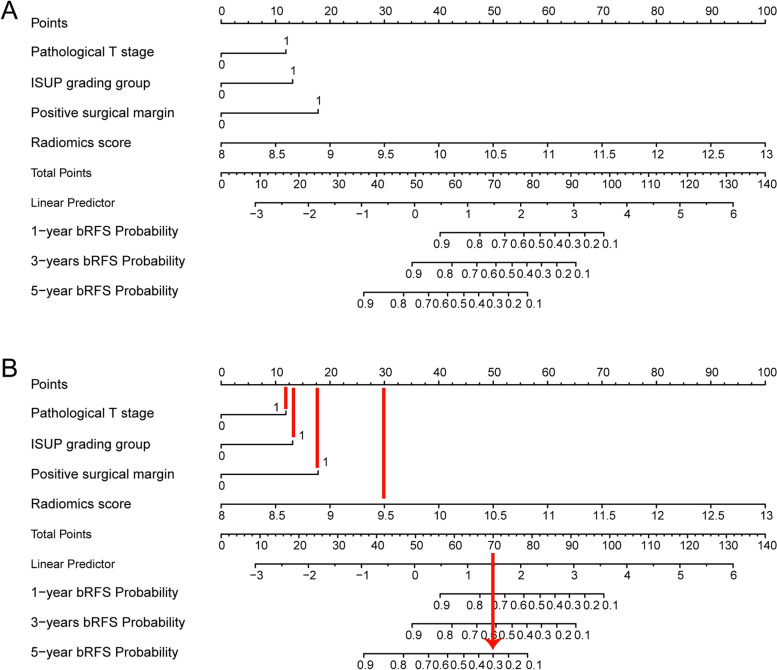
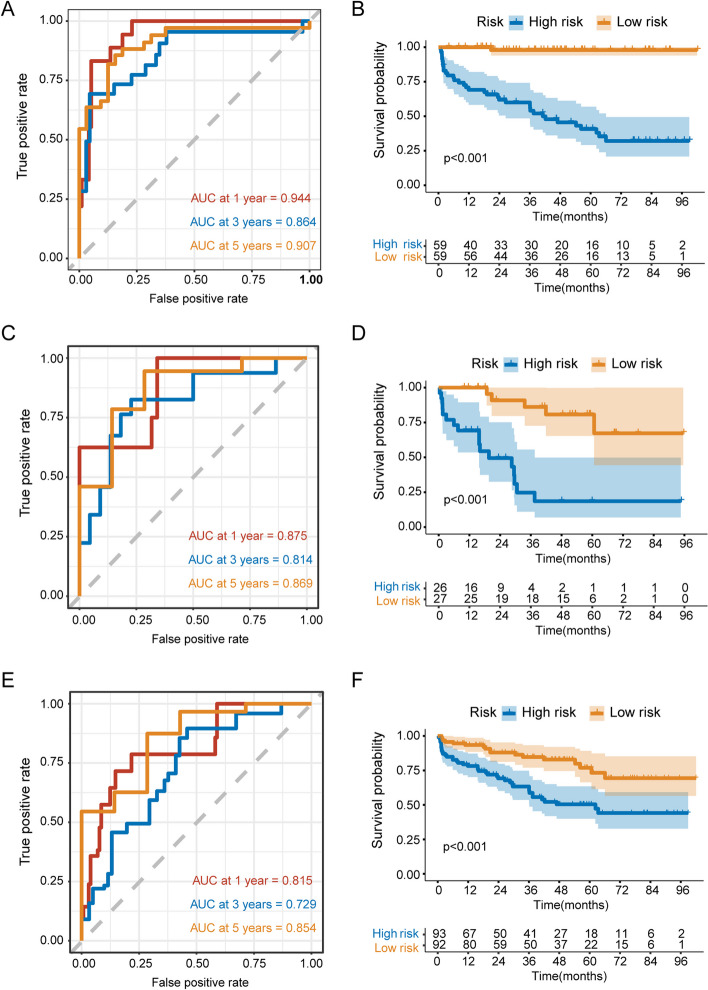
One hundred and twenty-one patients (33.98%) experienced biochemical recurrence. ROC analyses showed that the Area Under the Curve (AUC) of the periprostatic fat-intratumoral radiomics model demonstrated the highest AUC at 0.921 (95%CI, 0.857-0.981), 0.875 (95%CI, 0.763-0.950), 0.854 (95%CI, 0.706-0.923) for 1-year, 3-years and 5-years bRFS. Multivariate Cox regression analysis revealed that Pathological T stage, ISUP grading group and Positive surgical margin were independent prognostic factors for predicting bRFS. A radiomics-clinical nomogram based on these clinical predictors and periprostatic fat-intratumoral radiomics score was constructed. Kaplan-Meier analyses showed that radiomics-clinical nomogram was significantly related with survival of PCa (P < 0.001); and calibration curves revealed the predicted and observed survival probability of 1-year, 3-year and 5-year bRFS had high degree of consistency in the training and validation group. The radiomics-clinical nomogram showed a significant improvement than the clinical model for 1-year (AUC, 0.944; 95%CI, 0.912-0.990 vs. AUC, 0.839; 95%CI, 0.661-0.928; P = 0.009), 3-year (AUC, 0.864; 95%CI, 0.772-0.969 vs. AUC, 0.776; 95%CI, 0.602-0.872; P = 0.008), and 5-year bRFS (AUC, 0.907; 95%CI, 0.836-0.982 vs. AUC, 0.819; 95%CI, 0.687-0.915; P = 0.027).
This study developed and validated the radiomics-clinical nomogram for the prediction of bRFS in non-metastatic PCa patients underwent RP.
建立并验证基于前列腺周围脂肪磁共振成像(MRI)的放射组学列线图,以预测接受根治性前列腺切除术(RP)治疗的非转移性前列腺癌(PCa)患者的生化无复发生存率(bRFS)。
对在我院接受术前 mpMRI 检查并随后接受 RP 治疗的 356 例非转移性 PCa 患者进行回顾性研究。从 T2 加权成像(T2WI)和表观扩散系数(ADC)图像上勾画的肿瘤内区域和前列腺周围脂肪区域提取放射组学特征。应用最小绝对收缩和选择算子(LASSO)Cox 回归分析,构建三个放射组学模型,然后通过 Cox 风险回归分析,将最佳放射组学评分和临床病理危险因素相结合,构建一个联合放射组学-临床模型,绘制列线图。通过接受者操作特征(ROC)曲线、Kaplan-Meier 分析和校准曲线来评估预测性能。
121 例患者(33.98%)发生生化复发。ROC 分析显示,前列腺周围脂肪-肿瘤内放射组学模型的曲线下面积(AUC)在 1 年、3 年和 5 年 bRFS 中表现最佳,分别为 0.921(95%CI,0.857-0.981)、0.875(95%CI,0.763-0.950)和 0.854(95%CI,0.706-0.923)。多变量 Cox 回归分析显示,病理 T 分期、ISUP 分级组和阳性切缘是预测 bRFS 的独立预后因素。基于这些临床预测因素和前列腺周围脂肪-肿瘤内放射组学评分构建了一个放射组学-临床列线图。Kaplan-Meier 分析显示,放射组学-临床列线图与 PCa 患者的生存情况显著相关(P<0.001);校准曲线显示,1 年、3 年和 5 年 bRFS 的预测和观察生存概率在训练组和验证组中具有高度一致性。与临床模型相比,放射组学-临床列线图在 1 年(AUC,0.944;95%CI,0.912-0.990 vs. AUC,0.839;95%CI,0.661-0.928;P=0.009)、3 年(AUC,0.864;95%CI,0.772-0.969 vs. AUC,0.776;95%CI,0.602-0.872;P=0.008)和 5 年 bRFS(AUC,0.907;95%CI,0.836-0.982 vs. AUC,0.819;95%CI,0.687-0.915;P=0.027)方面均有显著改善。
本研究建立并验证了基于前列腺周围脂肪磁共振成像的放射组学-临床列线图,用于预测接受根治性前列腺切除术治疗的非转移性前列腺癌患者的生化无复发生存率。