Department of Cardiology, Health Science University, Istanbul Training and Research Hospital, Istanbul - Turquia.
Harran University, Faculty of Medicine, Department of Cardiology, Sanliurfa - Turquia.
Arq Bras Cardiol. 2024 Oct;121(11):e20240202. doi: 10.36660/abc.20240202.
Dual antiplatelet therapy (DAPT) is the treatment of choice for patients with acute and chronic coronary syndromes as it reduces mortality and prevents recurrent thrombotic complications. The assessment of both ischaemic burden and bleeding risk is crucial in deciding which DAPT to choose and how long it should be continued.
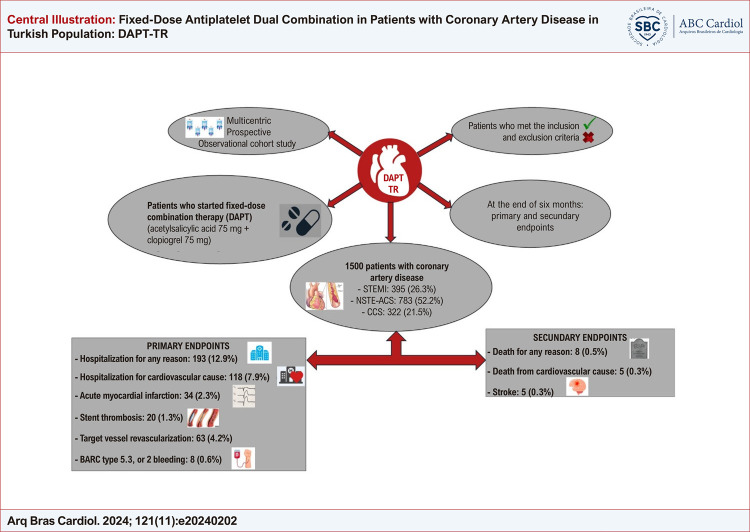
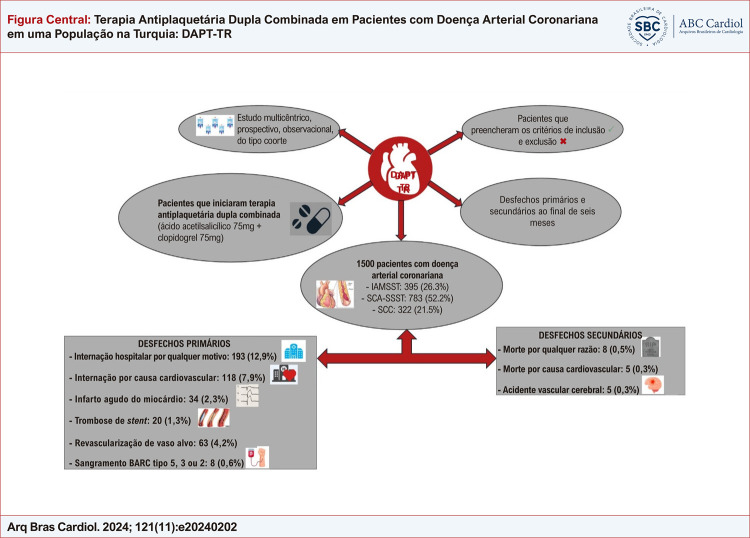
The aim of our study was to perform prospective clinical follow-up of patients receiving fixed-dose combination therapy (ASA 75 mg + clopidogrel 75 mg). Our study is a multicentric, cross-sectional, observational, cohort study.
A total of 1500 patients who were started on fixed-dose combination DAPT for acute or chronic coronary syndrome were included in the study. Primary endpoints were hospitalization for any reason, hospitalization for cardiovascular cause, acute myocardial infarction, stent thrombosis, target vessel revascularization and bleeding; the secondary endpoints were death for any reason or cardiovascular cause and stroke. The significance level adopted in the statistical analysis was 5%.
Median age was 63 years; 78.5% of the patients were receiving DAPT treatment for acute coronary syndrome. The rates of hospitalization for cardiovascular reasons, acute myocardial infartion, stent thrombosis and target-vessel revascularization were 7.9%, 2.3%, 1.3% and 4.2%, respectively. While the rate of BARC type 1 bleeding was 3.3%, the rate of BARC type 5, 3, or 2 bleeding was 0.6%. The secondary endpoints which were death from any cause, cardiovascular death and stroke were 0.5%, 0.3% and 0.3%, respectively. Conclusion: Our study shows that fixed-dose combination therapy is effective and safe in appropriately selected patients with acute or chronic coronary syndromes.
双联抗血小板治疗(DAPT)是急性和慢性冠状动脉综合征患者的首选治疗方法,可降低死亡率并预防复发性血栓并发症。评估缺血负担和出血风险对于选择哪种 DAPT 以及应持续多长时间至关重要。
我们的研究目的是对接受固定剂量联合治疗(ASA 75mg+氯吡格雷 75mg)的患者进行前瞻性临床随访。我们的研究是一项多中心、横断面、观察性、队列研究。
共纳入 1500 例因急性或慢性冠状动脉综合征开始接受固定剂量联合 DAPT 的患者。主要终点为因任何原因住院、因心血管原因住院、急性心肌梗死、支架血栓形成、靶血管血运重建和出血;次要终点为任何原因或心血管原因导致的死亡和卒中。统计分析中采用的显著性水平为 5%。
中位年龄为 63 岁;78.5%的患者因急性冠状动脉综合征接受 DAPT 治疗。因心血管原因住院、急性心肌梗死、支架血栓形成和靶血管血运重建的发生率分别为 7.9%、2.3%、1.3%和 4.2%。BARC 1 型出血发生率为 3.3%,BARC 5 型、3 型或 2 型出血发生率为 0.6%。次要终点为任何原因导致的死亡、心血管死亡和卒中的发生率分别为 0.5%、0.3%和 0.3%。结论:我们的研究表明,固定剂量联合治疗在适当选择的急性或慢性冠状动脉综合征患者中是有效且安全的。