Elsabani Elrasheed M, Badr Badr A, Dhalaan Mohammad, Alotaibi Anwar, Alrujaib Abdulrahman, Alahmed Rabab, Alabbadi Abdulrahman, Kheir Omer
Hospital Medicine, Johns Hopkins Aramco Healthcare, Dhahran, SAU.
Internal Medicine, Johns Hopkins Aramco Healthcare, Dhahran, SAU.
Cureus. 2024 Nov 28;16(11):e74684. doi: 10.7759/cureus.74684. eCollection 2024 Nov.
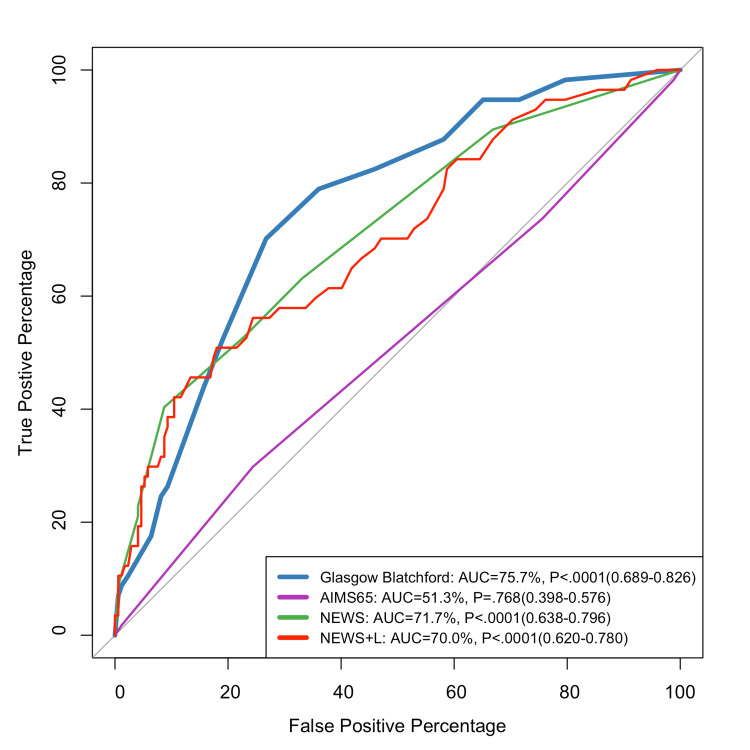
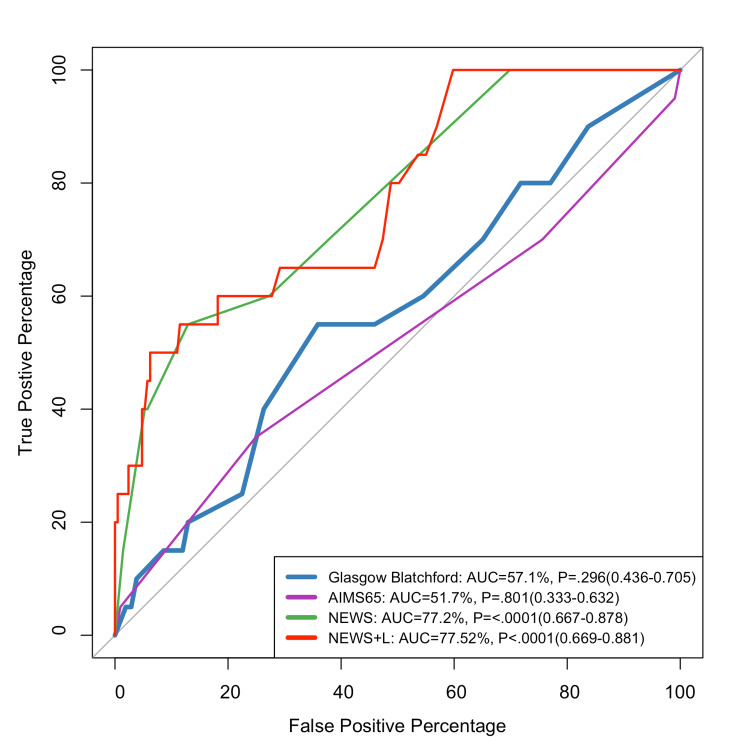
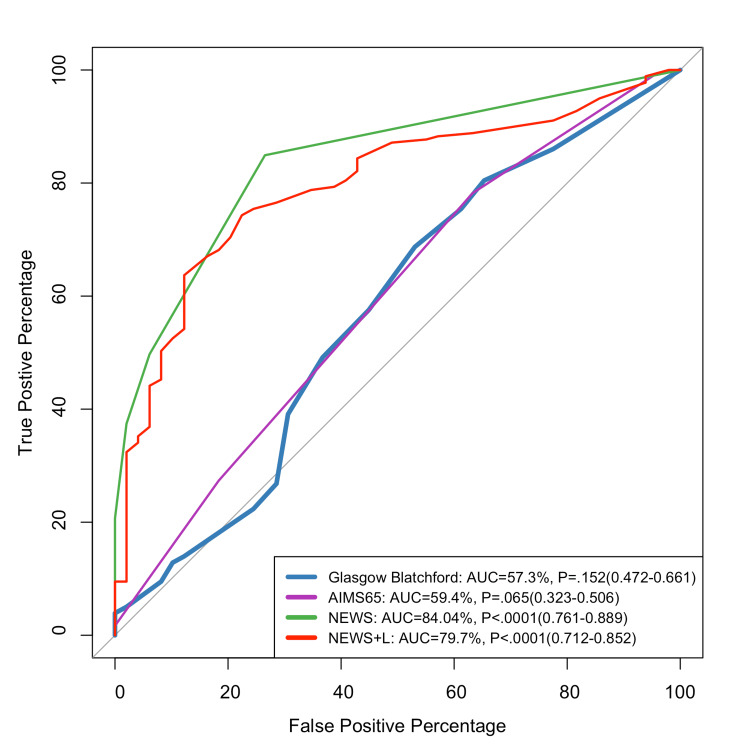
Introduction Upper gastrointestinal bleeding (UGIB) is a common medical emergency that causes significant deaths and morbidity. Effective risk classification is crucial for clinical decision-making and resource allocation. Several risk assessments, including the Glasgow-Blatchford score (GBS), AIMS65, National Early Warning Score (NEWS), and National Early Warning Score + Lactate (NEWS+L), are widely used, but each has unique strengths and disadvantages. The purpose of this study is to examine the predictive performance of different scoring systems for critical outcomes, including blood transfusion requirements, inpatient admission, and 90-day mortality, in patients with nonvariceal upper GI bleeding (NVUGIB). Method We performed a retrospective review of 229 individuals who presented with nonvariceal upper GI hemorrhage. Baseline demographics, clinical presentations, laboratory values, and vital signs were gathered. For each patient, GBS, AIMS65, NEWS, and NEWS+L scores were calculated. The predictive accuracy of these scores for blood transfusion, inpatient admission, and 90-day mortality was evaluated using the area under the receiver operating characteristic curves (AUCs). Results The results show that the GBS had the highest predictive accuracy for blood transfusion (AUC: 75.7%), while NEWS was the best predictor for inpatient admission (AUC: 84.04%). For 90-day mortality, NEWS and NEWS+L performed similarly, with AUCs of 77.25% and 77.52%, respectively. AIMS65 demonstrated low predictive capacity across outcomes, although it was less successful than other ratings for specific outcomes. Conclusion Our results show that each risk score has distinct predictive strengths: GBS for transfusion, NEWS for admission, and NEWS/NEWS+L for mortality. Combining these scores may improve risk classification and direct-focused therapies, hence improving patient outcomes in UGIB.
引言 上消化道出血(UGIB)是一种常见的医疗急症,会导致大量死亡和发病。有效的风险分类对于临床决策和资源分配至关重要。包括格拉斯哥 - 布拉奇福德评分(GBS)、AIMS65、国家早期预警评分(NEWS)和国家早期预警评分 + 乳酸(NEWS + L)在内的几种风险评估方法被广泛使用,但每种方法都有其独特的优缺点。本研究的目的是检验不同评分系统对非静脉曲张性上消化道出血(NVUGIB)患者的关键结局(包括输血需求、住院和90天死亡率)的预测性能。方法 我们对229例非静脉曲张性上消化道出血患者进行了回顾性研究。收集了基线人口统计学、临床表现、实验室值和生命体征。为每位患者计算GBS、AIMS65、NEWS和NEWS + L评分。使用受试者操作特征曲线下面积(AUC)评估这些评分对输血、住院和90天死亡率的预测准确性。结果 结果表明,GBS对输血的预测准确性最高(AUC:75.7%),而NEWS是住院的最佳预测指标(AUC:84.04%)。对于90天死亡率,NEWS和NEWS + L表现相似,AUC分别为77.25%和77.52%。AIMS65在所有结局中的预测能力较低,尽管在特定结局方面不如其他评分成功。结论 我们的结果表明,每个风险评分都有不同的预测优势:GBS用于输血,NEWS用于住院,NEWS/NEWS + L用于死亡率。结合这些评分可能会改善风险分类并指导针对性治疗,从而改善UGIB患者的结局。