Aredo Jacqueline V, Wakelee Heather A, Ramchandran Kavitha J, Neal Joel W, Diehn Maximilian, Hui Angela Bik-Yu, Salahudeen Ameen, Kwong Bernice, Berry Gerald J, Guo H Henry, Cunanan Kristen, Vali Shireen, Pancirer Danny, Tsang Vivian, Hwang Grace, Loza Monica, Johnson Brittany, Blanchard Isabelle, Padda Sukhmani K
Division of Oncology, Department of Medicine, Stanford Cancer Institute, Stanford University School of Medicine, Stanford, California.
Department of Radiation Oncology, Stanford Cancer Institute, Stanford University School of Medicine, Stanford, California.
JTO Clin Res Rep. 2024 Oct 17;5(12):100741. doi: 10.1016/j.jtocrr.2024.100741. eCollection 2024 Dec.
There are no standard targeted treatment options for advanced -mutant NSCLC beyond G12C inhibitors. A computational model identified regorafenib and low-dose methotrexate as synergistic in preclinical models of -mutant NSCLC. This study evaluated the efficacy and safety of the combination in previously treated advanced -mutant NSCLC.
This single-arm phase II study included regorafenib 80 to 120 mg oral daily and oral methotrexate dose escalated to tolerability from 10 to 20 mg twice weekly during the first cycle. Both agents were administered on weeks 1 to 3 of each 4-week cycle. The primary end point was progression-free survival.
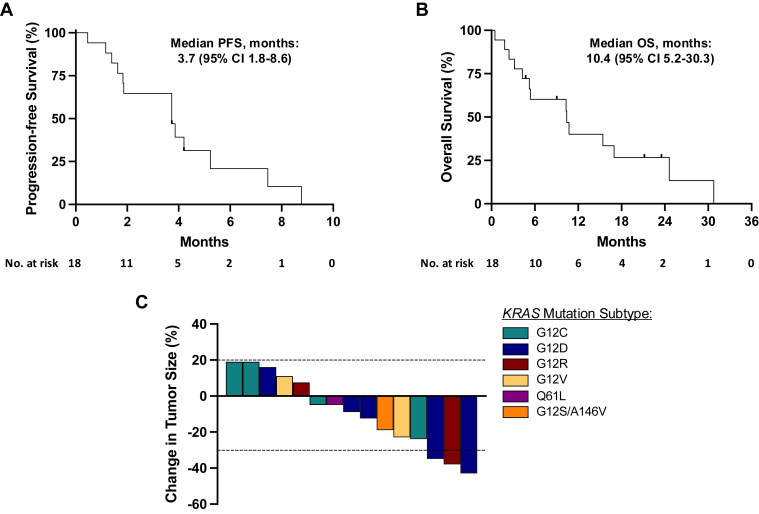
In total, 18 patients with -mutant NSCLC were enrolled. Five patients received regorafenib at a 120 mg starting dose with four discontinuing due to toxicity; subsequently, 13 patients were treated at an 80 mg starting dose, with eight dose-escalating to 120 mg after the first cycle. Median progression-free survival was 3.7 months (95% confidence interval 1.8-8.6) and median overall survival was 10.4 months (95% confidence interval 5.2-30.3). The objective response rate was 16.7% and the 8-week disease control rate was 66.7%. Grade 3 treatment-related adverse events occurred in 11 patients, most often oral mucositis (n = 2) and asymptomatic lipase increase (n = 2). One patient developed asymptomatic grade 4 lipase increase.
Combination treatment of regorafenib and oral methotrexate in patients with -mutant NSCLC was limited due to toxicity, and the study did not meet its primary end point. Computational modeling may aid in repurposing therapeutic options though caution must be exercised with tolerability.
除G12C抑制剂外,晚期KRAS突变型非小细胞肺癌(NSCLC)尚无标准的靶向治疗方案。一种计算模型确定瑞戈非尼和低剂量甲氨蝶呤在KRAS突变型NSCLC的临床前模型中具有协同作用。本研究评估了该联合方案在既往治疗过的晚期KRAS突变型NSCLC中的疗效和安全性。
这项单臂II期研究包括每日口服80至120毫克瑞戈非尼,在第一个周期内,口服甲氨蝶呤剂量从每周两次10毫克逐步递增至耐受剂量20毫克。两种药物均在每4周周期的第1至3周给药。主要终点是无进展生存期。
总共纳入了18例KRAS突变型NSCLC患者。5例患者起始剂量为120毫克瑞戈非尼,其中4例因毒性停药;随后,13例患者起始剂量为80毫克,8例在第一个周期后剂量递增至120毫克。中位无进展生存期为3.7个月(95%置信区间1.8 - 8.6),中位总生存期为10.4个月(95%置信区间5.2 - 30.3)。客观缓解率为16.7%,8周疾病控制率为66.7%。11例患者发生3级治疗相关不良事件,最常见的是口腔黏膜炎(n = 2)和无症状脂肪酶升高(n = 2)。1例患者出现无症状4级脂肪酶升高。
瑞戈非尼与口服甲氨蝶呤联合治疗KRAS突变型NSCLC患者因毒性受限,该研究未达到其主要终点。计算模型可能有助于重新利用治疗方案,但必须谨慎考虑耐受性。