Freiermuth Caroline E, Foster Jenny A, Manandhar Pratik, Arulraja Evangeline, Erkanli Alaattin, Pollack Charles V, Eucker Stephanie A
University of Cincinnati, Department of Emergency Medicine, Cincinnati, Ohio.
University of Cincinnati College of Medicine, Center for Addiction Research, Cincinnati, Ohio.
West J Emerg Med. 2024 Nov;25(6):875-882. doi: 10.5811/westjem.18380.
Pain is a major driver of visits to the emergency department (ED). Clinicians must consider not only the efficacy of treatment options but also subsequent healthcare utilization and patient-centered outcomes such as side effects from prescribed medications. Our goal in this study was to determine whether there was an association between acute pain treatment regimen (opioids, intranasal non-steroidal anti-inflammatory drugs [NSAIDs], or both) and unscheduled healthcare visits following ED discharge.
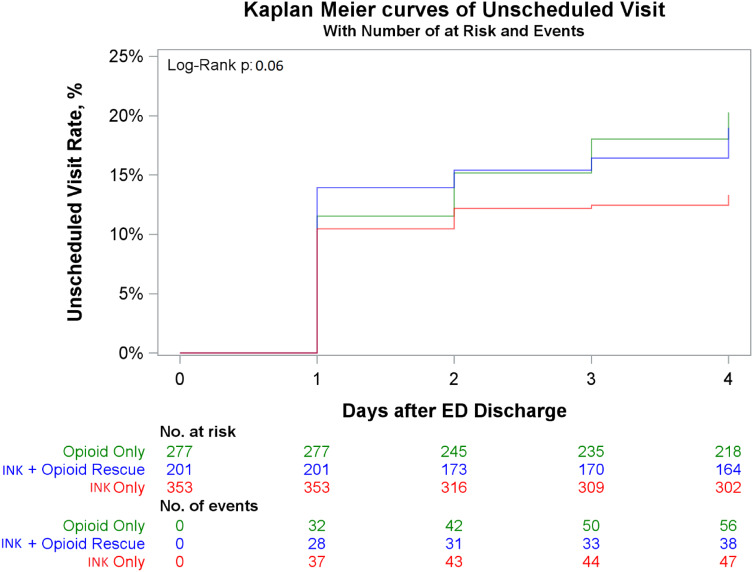
This study was a secondary analysis of the Acute Management of Pain from the Emergency Department (AMPED) prospective, observational cohort study. We used Cox proportional hazards analysis to assess the relationship between treatment regimen and time to first unscheduled healthcare visit. Repeated measures logistic regression analyses were used to determine the relationship between treatment regimen and any unscheduled visits, and to evaluate whether this relationship was mediated by pain severity and/or medication side effects.
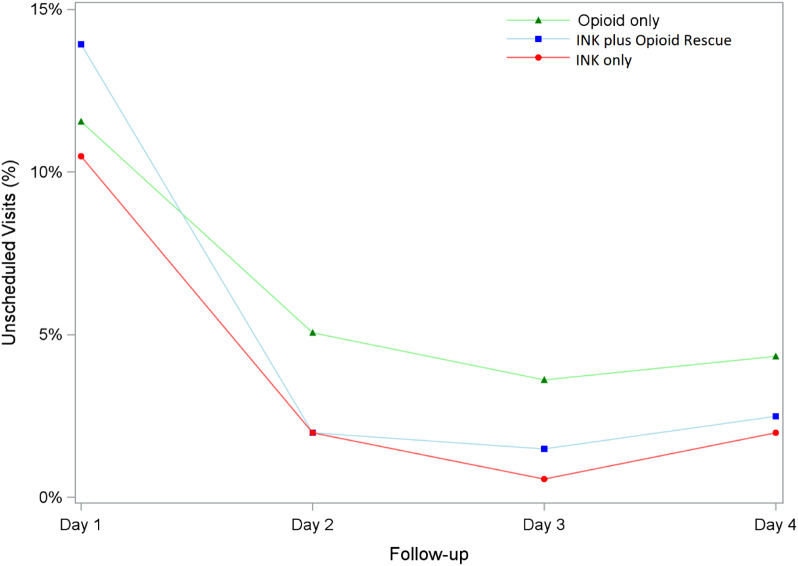
Of 831 total enrolled participants, 141 (16.9%) experienced an unplanned healthcare visit within five days of ED discharge. A majority of these visits happened one day after the ED visit. Those who were treated with intranasal NSAIDs only were less likely to have an unscheduled healthcare visit compared to those who received opioids only, with an adjusted odds ratio (AOR) of 0.63. The higher odds of unscheduled healthcare visits with opioids were mediated by both the presence of side effects and higher pain levels, with AORs of 2.24 and 1.33, respectively.
Opioid treatment for acute pain is associated with increased unscheduled healthcare visits compared to those treated with intranasal ketorolac. This difference can be explained by higher levels of ongoing pain and greater medication side effects.
疼痛是促使患者前往急诊科就诊的主要原因。临床医生不仅要考虑治疗方案的疗效,还要考虑后续的医疗保健利用情况以及以患者为中心的结果,如处方药的副作用。我们这项研究的目的是确定急性疼痛治疗方案(阿片类药物、鼻内非甾体抗炎药[NSAIDs]或两者皆用)与急诊出院后非计划的医疗就诊之间是否存在关联。
本研究是对急诊科疼痛急性管理(AMPED)前瞻性观察队列研究的二次分析。我们使用Cox比例风险分析来评估治疗方案与首次非计划医疗就诊时间之间的关系。重复测量逻辑回归分析用于确定治疗方案与任何非计划就诊之间的关系,并评估这种关系是否由疼痛严重程度和/或药物副作用介导。
在总共831名登记参与者中,141人(16.9%)在急诊出院后五天内经历了非计划的医疗就诊。这些就诊大多发生在急诊就诊后的一天。与仅接受阿片类药物治疗的患者相比,仅接受鼻内NSAIDs治疗的患者进行非计划医疗就诊的可能性较小,调整后的优势比(AOR)为0.63。使用阿片类药物导致非计划医疗就诊的较高几率是由副作用的存在和较高的疼痛水平介导的,AOR分别为2.24和1.33。
与接受鼻内酮咯酸治疗的患者相比,急性疼痛的阿片类药物治疗与增加非计划医疗就诊相关。这种差异可以通过持续较高的疼痛水平和更大的药物副作用来解释。