Houston A B, Simpson I A, Sheldon C D, Doig W B, Coleman E N
Br Heart J. 1986 Apr;55(4):381-4. doi: 10.1136/hrt.55.4.381.
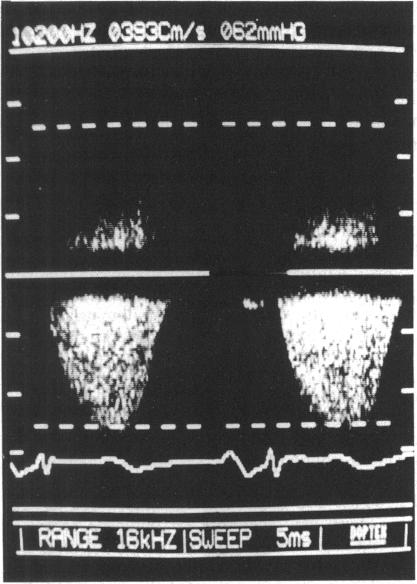
Pressure gradients estimated by Doppler echocardiography were compared with values obtained at cardiac catheterisation in 31 children (aged seven days to 16 years, mean 2 years 7 months) with pulmonary infundibular stenosis including 16 with tetralogy of Fallot. Various parasternal and subcostal positions were explored to obtain the maximum velocity of blood flow and the obstructive gradient was calculated from the modified Bernoulli formula. The gradient across the obstruction could be measured directly at the time of catheterisation in only 21 patients. The correlation coefficient for the Doppler and total measured gradients was r = 0.90 for catheter entry and r = 0.77 for catheter withdrawal. Doppler ultrasound, by measuring the total gradient from the right ventricle to the pulmonary artery, provides a non-invasive assessment of the severity of pulmonary stenosis, and in those with infundibular obstruction allowance need not be made for possible energy losses caused by the elongated obstruction or the presence of narrowing at more than one level.
对31例患有肺动脉漏斗部狭窄的儿童(年龄7天至16岁,平均2岁7个月)进行了研究,通过多普勒超声心动图估算的压力梯度与心导管检查获得的值进行了比较,其中包括16例法洛四联症患儿。探索了各种胸骨旁和肋下位置以获得血流的最大速度,并根据改良的伯努利公式计算梗阻梯度。仅21例患者在导管插入时能够直接测量梗阻两端的压力梯度。导管插入时,多普勒测量的压力梯度与总测量压力梯度的相关系数r = 0.90,导管拔出时r = 0.77。多普勒超声通过测量从右心室到肺动脉的总压力梯度,对肺动脉狭窄的严重程度提供了一种非侵入性评估,对于漏斗部梗阻患者,无需考虑因梗阻延长或多个层面存在狭窄可能导致的能量损失。