Whitehouse Daniel P, Wilson Lindsay, Czeiter Endre, Buki Andras, Wang Kevin K W, von Steinbüchel Nicole, Zeldovich Marina, Steyerberg Ewout, Maas Andrew I R, Menon David K, Newcombe Virginia F J
From the Perioperative, Acute, Critical Care and Emergency Medicine (PACE) (D.P.W., D.M., V.F.J.N.), Department of Medicine, University of Cambridge, Addenbrooke's Hospital; Division of Psychology (L.W.), University of Stirling, United Kingdom; Department of Neurosurgery (E.C.), Medical School, and Neurotrauma Research Group (E.C.), Szentagothai Research Centre, University of Pecs, Hungary; Department of Neurosurgery (A.B.), Faculty of Medicine and Health, Örebro University, Sweden; Department of Neurobiology (K.K.W.W.), Center for Neurotrauma, Multiomics & Biomarkers (CNMB) Neuroscience Institute, Morehouse School of Medicine (MSM), Atlanta, GA; Program for Neurotrauma, Neuroproteomics and Biomarker Research (K.K.W.W.), Departments of Emergency Medicine, Psychiatry and Neuroscience, University of Florida, McKnight Brain Institute, Gainesville; Institute of Psychology (N.v.S., M.Z.), University of Innsbruck; Faculty of Psychotherapy Science (M.Z.), Sigmund Freud University, Vienna, Austria; Department of Biomedical Data Sciences (E.S.), Leiden University Medical Center, the Netherlands; Department of Neurosurgery (A.I.R.M.), Antwerp University Hospital, Edegem; and Department of Translational Neuroscience (A.I.R.M.), Faculty of Medicine and Health Science, University of Antwerp, Belgium.
Neurology. 2025 Jan 14;104(1):e210040. doi: 10.1212/WNL.0000000000210040. Epub 2024 Dec 9.
There is seemingly contradictory evidence concerning relationships between day-of-injury biomarkers and outcomes after mild traumatic brain injury (mTBI). To address this issue, we examined the association between a panel of biomarkers and multidimensional TBI outcomes.
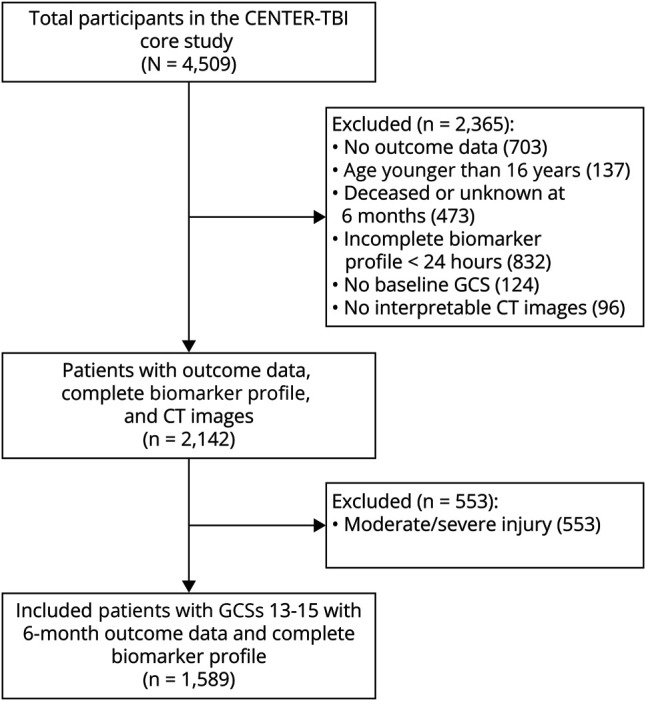
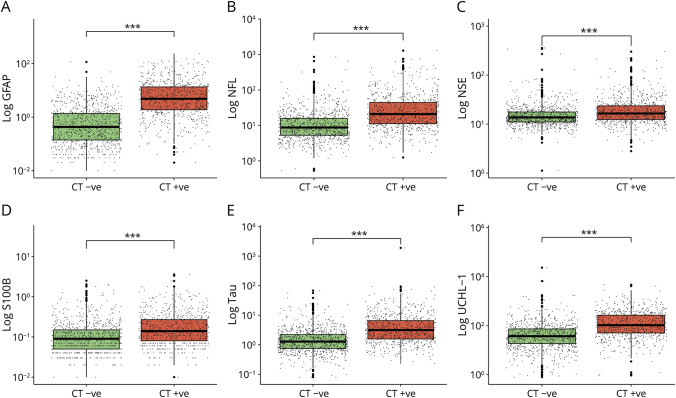
Participants with mTBI (Glasgow coma scores [GCSs] 13-15) were selected from Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury, a European observational study recruiting patients with TBI with indication for brain CT and presentation within 24 hours. Exclusion criteria for this secondary analysis were age younger than 16 years, incomplete biomarker panel, death, or no recorded outcomes. Participants were separated into 2 groups, CT-negative and CT-positive. Multivariable binary logistic regression was used to assess the relation between the log biomarker level (glial fibrillary acidic protein [GFAP], neurofilament light [NfL], neuron-specific enolase [NSE], S100 calcium-binding protein B [S100B], tau, ubiquitin C-terminal hydrolase L1 [UCH-L1]) and dichotomized 6-month outcomes (functional outcomes [GOSE score <8], health-related quality of life [HRQoL; Quality of Life after Brain Injury-Overall Scale (QOLIBRI-OS) score <52, Short-Form 12-Item Survey version 2 Mental Component Summary (SF12v2 MCS) score <40, Short-Form 12-Item Survey version 2 Physical Component Summary (SF12v2 PCS) score <40], persistent postconcussion symptoms [Rivermead Post-Concussion Symptoms Questionnaire score ≥16], anxiety disorder [Generalized Anxiety Disorder-7 (GAD-7) score ≥8], depression [Patient Health Questionnaire-9 (PHQ-9) score ≥10], and post-traumatic stress disorder [PTSD Checklist for DSM-5 (PCL-5) score ≥33]).
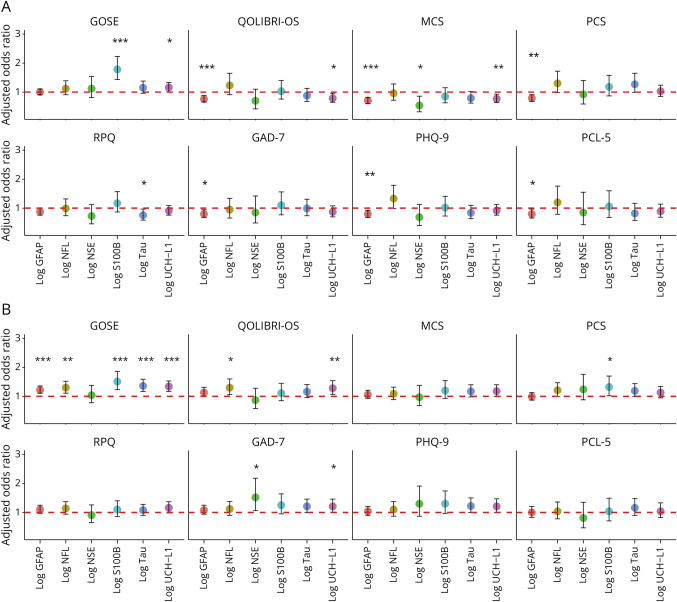
A total of 1,589 participants (865 CT-negative, 724 CT-positive) were included (77% GCS 15, median age 52 years, 66% male). Higher biomarker levels were associated with a GOSE score <8: CT-negative: S100B (odds ratio [OR] 1.78, 95% CI 1.43-2.23) and UCH-L1 (OR 1.16, 95% CI 1.01-1.33); CT-positive: GFAP (OR 1.22, 95% CI 1.11-1.36), NfL (OR 1.30, 95% CI 1.11-1.52), S100B (OR 1.51, 95% CI 1.23-1.86), tau (OR 1.36, 95% CI 1.17-1.59), and UCH-L1 (OR 1.34, 95% CI 1.17-1.53). In CT-positive participants, positive association was seen between NfL (OR 1.3, 95% CI 1.06-1.60) and UCH-L1 (OR 1.28, 95% CI 1.07-1.54) with QOLIBRI-OS; S100B (OR 1.32, 95% CI 1.02-1.70) with SF12v2 PCS; and NSE (OR 1.52, 95% CI 1.06-2.18) and UCH-L1 (OR 1.21, 95% CI 1.01-1.46) with the GAD-7. However, in CT-negative participants only, negative associations were seen between GFAP and impairment on the QOLIBRI-OS (OR 0.76, 95% CI 0.66-0.88), SF12v2 MCS (OR 0.71, 95% CI 0.61-0.82), SF12v2 PCS (OR 0.79, 95% CI 0.68-0.91), GAD-7 (OR 0.80, 0.68-0.95), PHQ-9 (OR 0.80, 95% CI 0.68-0.93), and PCL-5 (OR 0.80, 95% CI 0.66-0.97).
Participants with higher biomarker levels had greater odds of impaired functional recovery. However, in CT-negative participants, higher GFAP concentrations were associated with better HRQoL and less impaired mental health. Further exploration is required of the patient phenotypes that may explain the relationships observed in this analysis.
关于轻度创伤性脑损伤(mTBI)后损伤当日生物标志物与预后之间的关系,现有证据似乎相互矛盾。为解决这一问题,我们研究了一组生物标志物与多维TBI预后之间的关联。
从欧洲创伤性脑损伤协作神经创伤有效性研究中选取mTBI患者(格拉斯哥昏迷评分[GCS]为13 - 15分),这是一项欧洲观察性研究,招募有脑CT检查指征且在伤后24小时内就诊的TBI患者。本次二次分析的排除标准为年龄小于16岁、生物标志物检测不全、死亡或无记录的预后情况。参与者被分为两组,CT阴性组和CT阳性组。采用多变量二元逻辑回归评估生物标志物水平对数(胶质纤维酸性蛋白[GFAP]、神经丝轻链[NfL]、神经元特异性烯醇化酶[NSE]、S100钙结合蛋白B[S100B]、tau蛋白、泛素C末端水解酶L1[UCH - L1])与6个月二分法预后(功能预后[GOSE评分<8]、健康相关生活质量[HRQoL;脑损伤后生活质量总体量表(QOLIBRI - OS)评分<52、简明健康调查问卷第2版12项心理成分总结(SF12v2 MCS)评分<40、简明健康调查问卷第2版12项身体成分总结(SF12v2 PCS)评分<40]、持续性脑震荡后症状[Rivermead脑震荡后症状问卷评分≥16]、焦虑症[广泛性焦虑障碍量表 - 7(GAD - 7)评分≥8]、抑郁症[患者健康问卷 - 9(PHQ - 9)评分≥10]以及创伤后应激障碍[精神疾病诊断与统计手册第5版创伤后应激障碍检查表(PCL - 5)评分≥33])之间的关系。
共纳入1589名参与者(865名CT阴性,724名CT阳性)(77%的GCS评分为15分,中位年龄52岁,66%为男性)。较高的生物标志物水平与GOSE评分<8相关:CT阴性组:S100B(比值比[OR]1.78,95%置信区间[CI]1.43 - 2.23)和UCH - L1(OR 1.16,95% CI 1.01 - 1.33);CT阳性组:GFAP(OR 1.22,95% CI 1.11 - 1.36)、NfL(OR 1.30,95% CI 1.11 - 1.52)、S100B(OR 1.51,95% CI 1.23 - 1.86)、tau蛋白(OR 1.36,95% CI 1.17 - 1.59)和UCH - L1(OR 1.34,95% CI 1.17 - 1.53)。在CT阳性参与者中,NfL(OR 1.3,95% CI 1.06 - 1.60)和UCH - L1(OR 1.28,95% CI 1.07 - 1.54)与QOLIBRI - OS呈正相关;S100B(OR 1.32,95% CI 1.02 - 1.70)与SF12v2 PCS呈正相关;NSE(OR 1.52,95% CI 1.06 - 2.18)和UCH - L1(OR 1.21,95% CI 1.01 - 1.46)与GAD - 7呈正相关。然而,仅在CT阴性参与者中,GFAP与QOLIBRI - OS(OR 0.76,95% CI 0.66 - 0.88)、SF12v2 MCS(OR 0.71,95% CI 0.61 - 0.82)、SF12v2 PCS(OR 0.79,95% CI 0.68 - 0.91)、GAD - 7(OR 0.80,0.68 - 0.95)、PHQ - 9(OR 0.80,95% CI 0.68 - 0.93)以及PCL - 5(OR 0.80,95% CI 0.66 - 0.97)的损伤呈负相关。
生物标志物水平较高的参与者功能恢复受损的几率更大。然而,在CT阴性参与者中,较高的GFAP浓度与更好的HRQoL和较轻的心理健康损害相关。需要进一步探索可能解释本分析中观察到的关系的患者表型。