Fuchs Kyra J, Göransson Marcus, Kester Michel G D, Ettienne Natasja W, van de Meent Marian, de Jong Rob C M, Koster Eva A S, Halkes Constantijn J M, Scheeren Ferenc, Heemskerk Mirjam H M, van Balen Peter, Falkenburg J H Frederik, Hadrup Sine R, Griffioen Marieke
Department of Hematology, Leiden University Medical Center, Leiden, The Netherlands.
Department of Health Technology, Technical University of Denmark, Lyngby, Denmark.
J Immunother Cancer. 2024 Dec 9;12(12):e009564. doi: 10.1136/jitc-2024-009564.
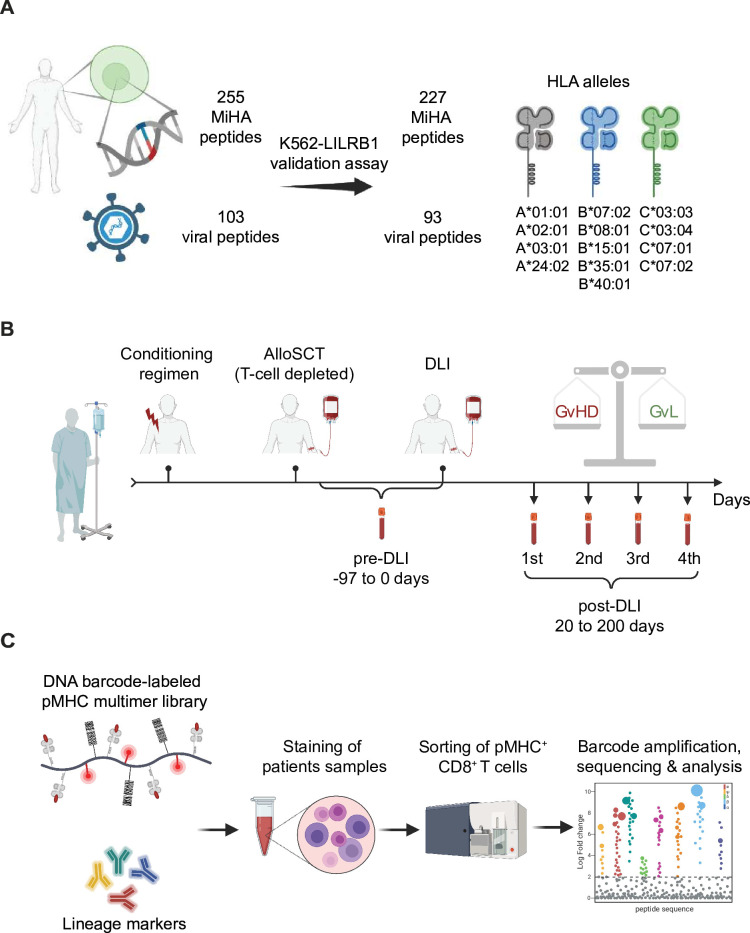
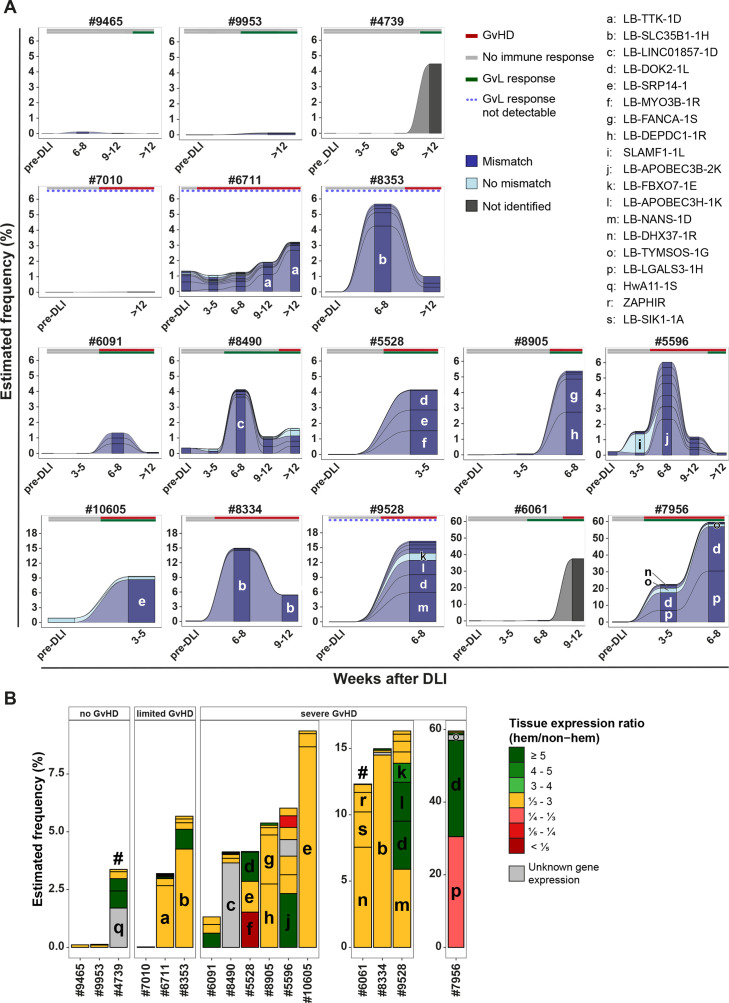
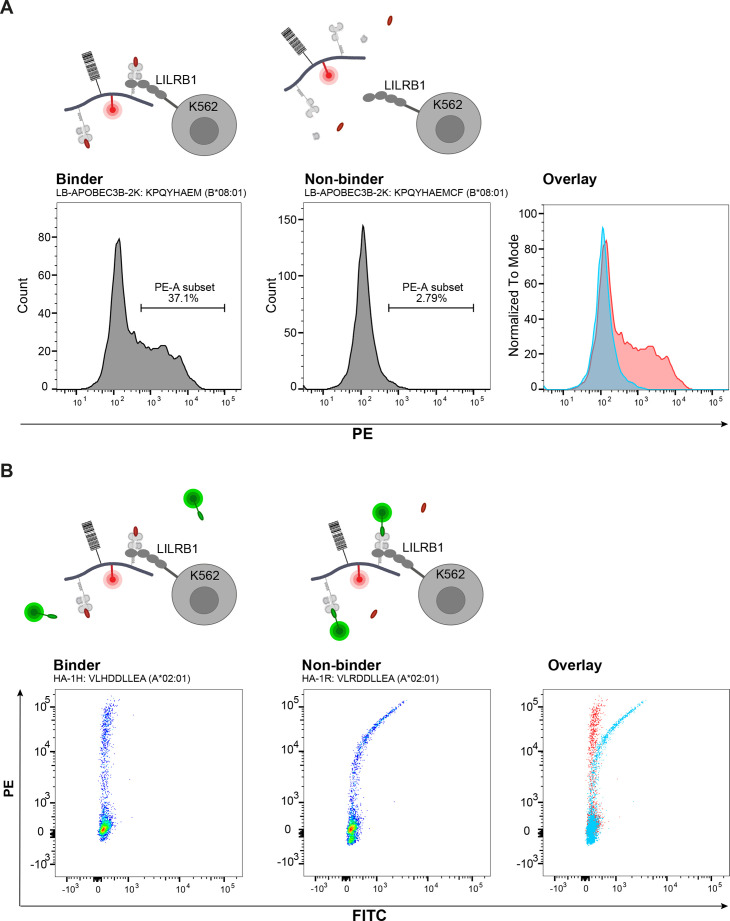
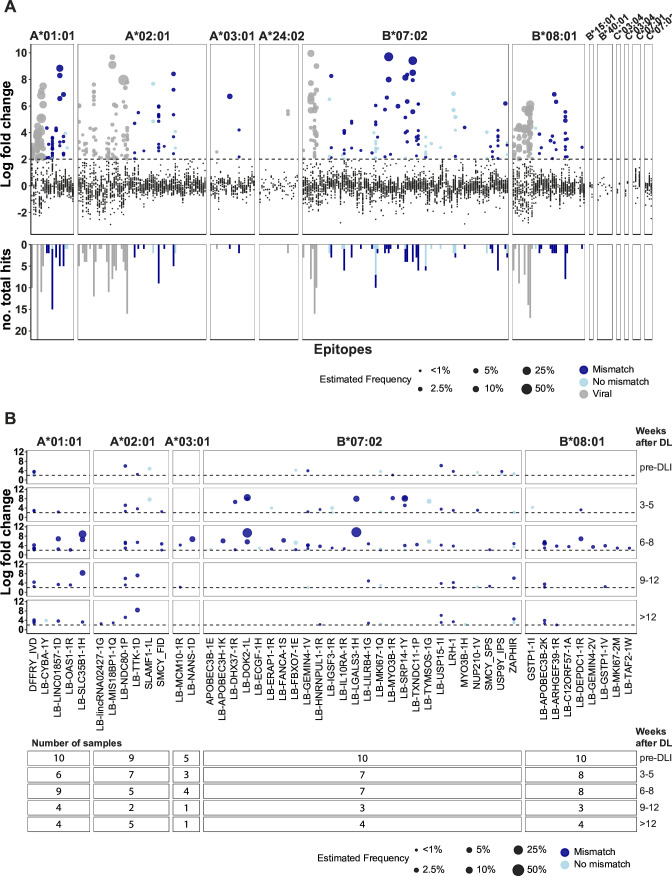
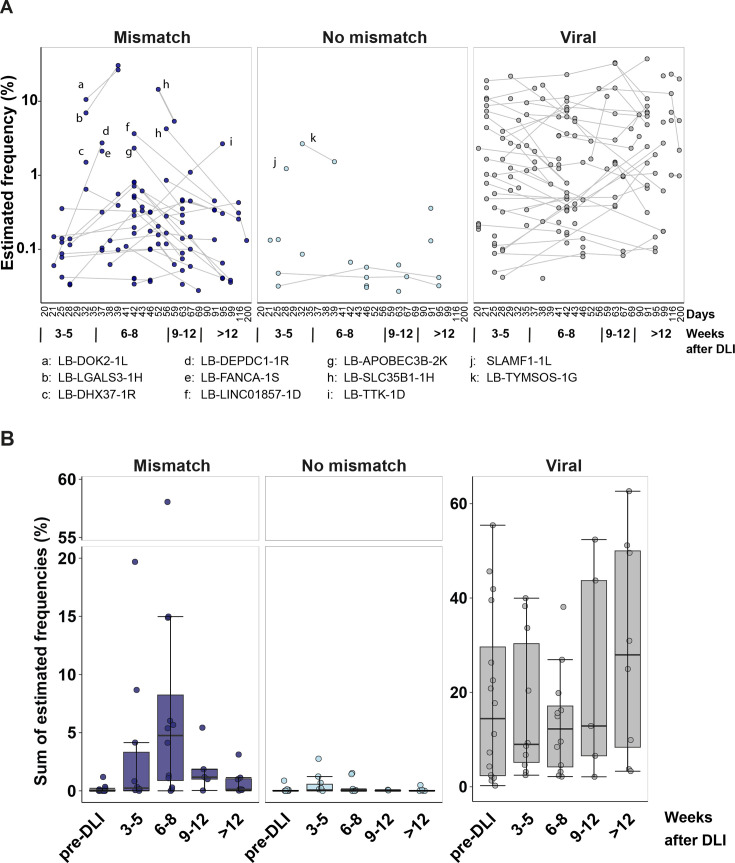
Allogeneic stem cell transplantation (alloSCT) provides a curative treatment option for hematological malignancies. After HLA-matched alloSCT, donor-derived T cells recognize minor histocompatibility antigens (MiHAs), which are polymorphic peptides presented by HLA on patient cells. MiHAs are absent on donor cells due to genetic differences between patient and donor. T cells targeting broadly expressed MiHAs induce graft-versus-leukemia (GvL) reactivity as well as graft-versus-host disease (GvHD), while T cells for MiHAs with restricted or preferential expression on hematopoietic or non-hematopoietic cells may skew responses toward GvL or GvHD, respectively. Besides tissue expression, overall strength of GvL and GvHD is also determined by T-cell frequencies against MiHAs.Here, we explored the use of DNA barcode-labeled peptide-MHC multimers to detect and monitor antigen-specific T cells for the recently expanded repertoire of HLA-I-restricted MiHAs. In 16 patients who experienced an immune response after donor lymphocyte infusion, variable T-cell frequencies up to 30.5% of CD8 T cells were measured for 49 MiHAs. High T-cell frequencies above 1% were measured in 12 patients for 19 MiHAs, with the majority directed against mismatched MiHAs, typically 6-8 weeks after donor lymphocyte infusion and at the onset of GvHD. The 12 patients included 9 of 10 patients with severe GvHD, 2 of 3 patients with limited GvHD and 1 of 3 patients without GvHD.In conclusion, we demonstrated that barcoded peptide-MHC multimers reliably detect and allow monitoring for MiHA-specific T cells during treatment to investigate the kinetics of immune responses and their impact on development of GvL and GvHD after HLA-matched alloSCT.
异基因干细胞移植(alloSCT)为血液系统恶性肿瘤提供了一种治愈性治疗选择。在 HLA 匹配的 alloSCT 后,供体来源的 T 细胞识别次要组织相容性抗原(MiHA),这些抗原是 HLA 在患者细胞上呈递的多态性肽段。由于患者和供体之间的基因差异,MiHA 在供体细胞上不存在。靶向广泛表达的 MiHA 的 T 细胞可诱导移植物抗白血病(GvL)反应以及移植物抗宿主病(GvHD),而针对在造血或非造血细胞上有受限或优先表达的 MiHA 的 T 细胞可能分别使反应偏向 GvL 或 GvHD。除了组织表达外,GvL 和 GvHD 的总体强度还由针对 MiHA 的 T 细胞频率决定。在此,我们探索了使用 DNA 条形码标记的肽 - MHC 多聚体来检测和监测针对最近扩展的 HLA - I 类限制性 MiHA 库的抗原特异性 T 细胞。在 16 例供体淋巴细胞输注后出现免疫反应的患者中,针对 49 种 MiHA 测量到可变的 T 细胞频率,高达 CD8 T 细胞的 30.5%。12 例患者针对 19 种 MiHA 测量到高于 1%的高 T 细胞频率,大多数针对不匹配的 MiHA,通常在供体淋巴细胞输注后 6 - 8 周以及 GvHD 发作时。这 12 例患者包括 10 例严重 GvHD 患者中的 9 例、3 例轻度 GvHD 患者中的 2 例以及 3 例无 GvHD 患者中的 1 例。总之,我们证明了条形码肽 - MHC 多聚体在治疗期间能够可靠地检测并监测 MiHA 特异性 T 细胞,以研究免疫反应的动力学及其对 HLA 匹配的 alloSCT 后 GvL 和 GvHD 发展的影响。