van Dam Cornelis Jan, Kramers Cornelis, Schellekens Arnt, Bouvy Marcel, van Dorp Eveline, Kowal Mikael A, Olofsen Erik, Dahan Albert, Niesters Marieke, van Velzen Monique
Tackling and Preventing the Opioid Epidemic (TAPTOE) Consortium, Utrecht, Netherlands.
Department of Anesthesiology, Leiden University Medical Center, Leiden, Netherlands.
Front Pain Res (Lausanne). 2024 Nov 25;5:1497111. doi: 10.3389/fpain.2024.1497111. eCollection 2024.
We determined whether adding cannabis to oxycodone for chronic non-cancer pain management could reduce treatment-related adverse effects (AEs) while maintaining effective analgesia.
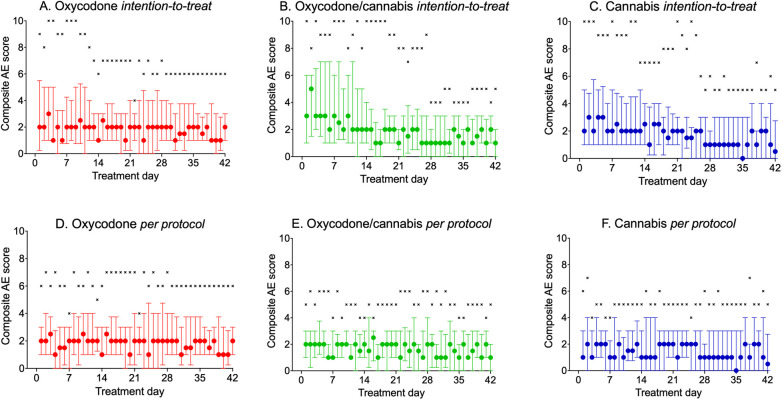
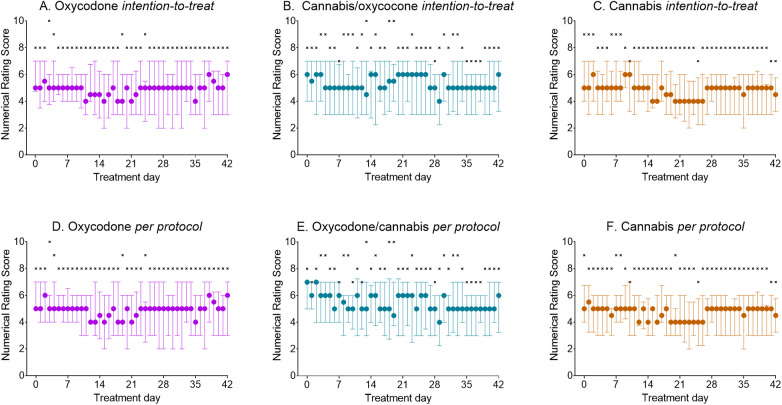
In this open-label study, fibromyalgia patients aged ≥18 years were randomized to receive 5 mg oxycodone tablets (max. four times/day), 150 mg of inhaled cannabis containing 6.3% Δ-tetrahydrocannabinol and 8% cannabidiol (max. times inhalation sessions/day), or a combination of both for 6 weeks. The primary endpoint was treatment-related adverse events, assessed using a 10-point composite adverse event (cAE) score; additionally, we recorded daily reported pain relief and daily tablet and cannabis consumption.
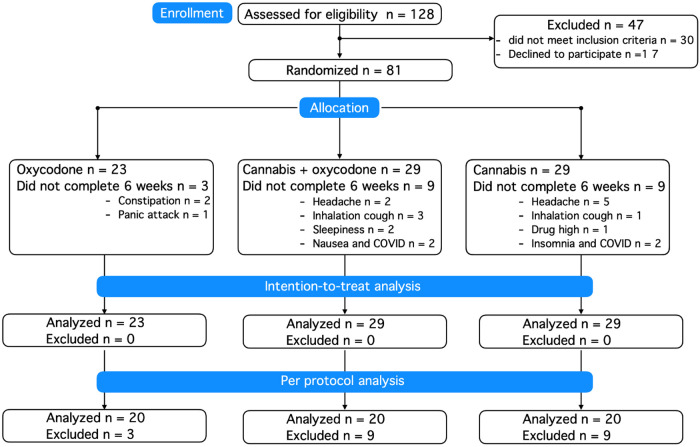
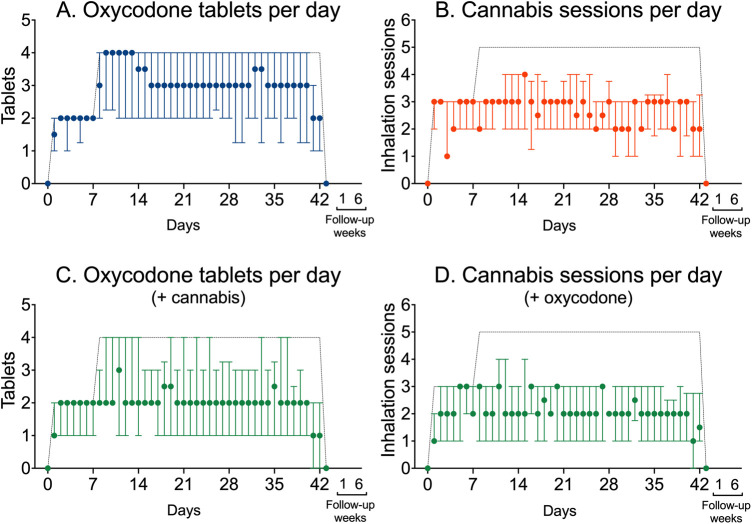
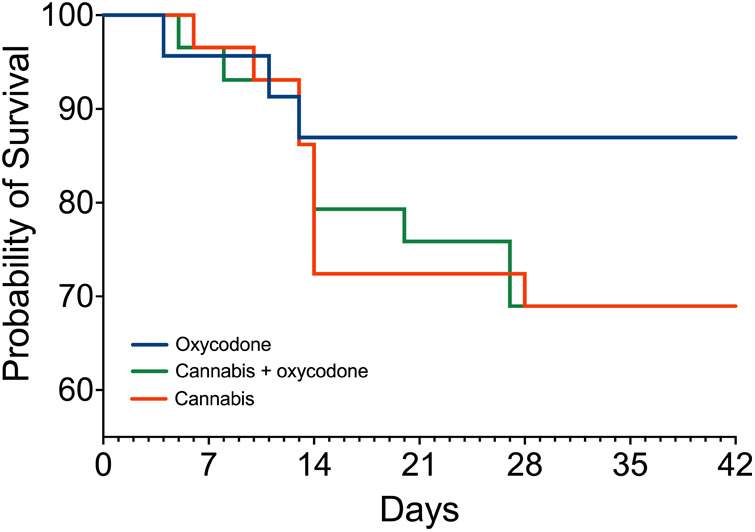
In total, 23 patients were treated with oxycodone, 29 with cannabis, and 29 with the oxycodone/cannabis combination. Three patients from the oxycodone group (13%) and 18 patients from the cannabis groups (31%, 9 in each group) withdrew from the trial within 2-3 weeks because of the severity of AEs. There were no differences in treatment-related cAE scores among the three groups that completed the study ( = 0.70). The analgesic responder rate showed a ≥1- point reduction in pain in 50% and a ≥2-point reduction in 20% of patients, while 50% of patients experienced no treatment benefit. The combination treatment reduced oxycodone tablet consumption by 35% ( = 0.02), but it did not affect the number of cannabis inhalation sessions.
Cannabis combined with oxycodone offered no advantage over either treatment alone, except for a reduction in opioid tablet intake; however, the overall drug load was the highest in the combination group. Moreover, cannabis was poorly tolerated and led to treatment discontinuation in one-third of participants treated with cannabis.
The trial was registered at the WHO International Clinical Trials Registry Platform (trialsearch.who.int) on July 26, 2019, identifier NL7902.
我们确定了在慢性非癌性疼痛管理中,将大麻添加到羟考酮中是否能在维持有效镇痛的同时减少与治疗相关的不良反应(AE)。
在这项开放标签研究中,年龄≥18岁的纤维肌痛患者被随机分为接受5毫克羟考酮片(最大每日4次)、含6.3% Δ-四氢大麻酚和8%大麻二酚的150毫克吸入式大麻(最大每日吸入次数)或两者联合使用6周。主要终点是与治疗相关的不良事件,使用10分综合不良事件(cAE)评分进行评估;此外,我们记录了每日报告的疼痛缓解情况以及每日的片剂和大麻消耗量。
总共,23名患者接受羟考酮治疗,29名接受大麻治疗,29名接受羟考酮/大麻联合治疗。羟考酮组有3名患者(13%)和大麻组有18名患者(31%,每组9名)因不良反应严重在2至3周内退出试验。完成研究的三组患者中,与治疗相关的cAE评分没有差异(=0.70)。镇痛有效率显示,50%的患者疼痛减轻≥1分,20%的患者疼痛减轻≥2分,而50%的患者未从治疗中获益。联合治疗使羟考酮片消耗量减少了35%(=0.02),但不影响大麻吸入次数。
大麻与羟考酮联合使用相比单独使用任何一种治疗方法均无优势,除了阿片剂摄入量减少;然而,联合组的总体药物负荷最高。此外,大麻耐受性差,导致三分之一接受大麻治疗的参与者停药。
该试验于2019年7月26日在世界卫生组织国际临床试验注册平台(trialsearch.who.int)注册,标识符为NL7902。