Catozzi Giulia, Pozzi Tommaso, Nocera Domenico, Donati Beatrice, Giovanazzi Stefano, Ghidoni Valentina, Galizia Mauro, D'Albo Rosanna, Busana Mattia, Romitti Federica, Gatta Alessandro, Moerer Onnen, Meissner Konrad, Quintel Michael, Herrmann Peter, Chiumello Davide, Camporota Luigi, Gattinoni Luciano
Department of Anaesthesiology, University Medical Center Göttingen, Göttingen, Germany.
Department of Health Sciences, University of Milan, Milan, Italy.
Intensive Care Med. 2025 Jan;51(1):62-71. doi: 10.1007/s00134-024-07712-0. Epub 2024 Dec 11.
The selection and intensity of respiratory support for ARDS are guided by PaO/FiO. However, ventilator-induced lung injury (VILI) is linked to respiratory mechanics and ventilator settings. We explored whether the VILI risk is related to ARDS severity based on oxygenation.
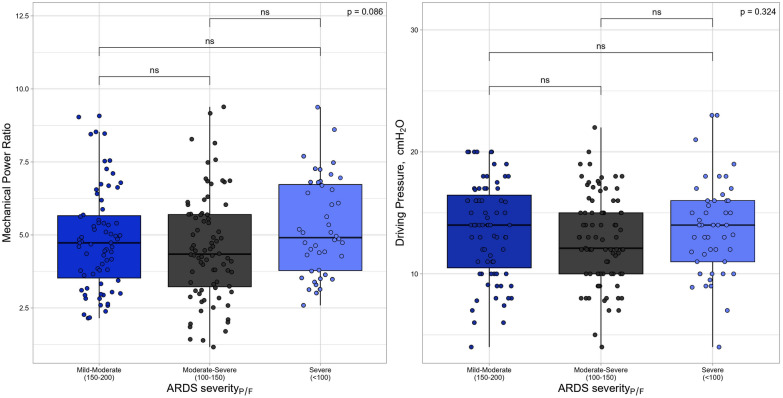
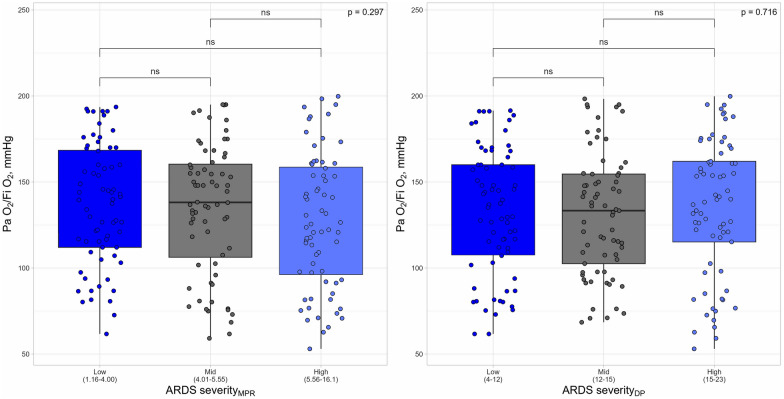
We analysed data on 228 ARDS subjects with PaO/FiO < 200 mmHg, categorized into three severity groups: one based on PaO/FiO ratio, and the others based on tertiles of predictors of VILI: mechanical power ratio (MPR) and driving pressure (DP). In each group of oxygenation-based ARDS severity and MPR and DP tertiles, we measured CT anatomy, gas exchange, respiratory mechanics, VILI prerequisites (lung elastance and lung gas volume), and VILI determinants (tidal volume, PEEP, airway pressures).
Predictors of VILI, such as MPR and DP, were similar across ARDS severity groups based on PaO/FiO ratio, while oxygenation remained comparable across different levels of VILI risk defined by MPR and DP. Oxygenation impairment was associated with increased lung weight, recruitability, and reduced well-inflated tissue. In contrast, MPR and DP tertiles affected variables associated with the baby lung size, such as lung gas volume and well-inflated tissue. Mechanical ventilation intensity increased progressively across MPR and DP tertiles, but remained similar across PaO/FiO severity groups.
ARDS severity based on oxygenation impairment does not reflect the prerequisites and determinants of VILI. This should prompt a reconsideration of recommending respiratory support based on oxygenation impairment, rather than VILI determinants.
急性呼吸窘迫综合征(ARDS)呼吸支持的选择和强度由动脉血氧分压/吸入氧分数值(PaO/FiO)指导。然而,呼吸机诱导的肺损伤(VILI)与呼吸力学和呼吸机设置有关。我们探讨了基于氧合的VILI风险是否与ARDS严重程度相关。
我们分析了228例PaO/FiO<200 mmHg的ARDS患者的数据,将其分为三个严重程度组:一组基于PaO/FiO比值,另外两组基于VILI预测指标的三分位数:机械功率比(MPR)和驱动压(DP)。在基于氧合的ARDS严重程度、MPR和DP三分位数的每组中,我们测量了CT解剖结构、气体交换、呼吸力学、VILI先决条件(肺弹性和肺气体容积)以及VILI决定因素(潮气量、呼气末正压、气道压力)。
基于PaO/FiO比值的ARDS严重程度组中,VILI的预测指标如MPR和DP相似,而在由MPR和DP定义的不同VILI风险水平下,氧合情况保持相当。氧合障碍与肺重量增加、可复张性增加以及充气良好的组织减少有关。相比之下,MPR和DP三分位数影响与小肺大小相关的变量,如肺气体容积和充气良好的组织。机械通气强度在MPR和DP三分位数中逐渐增加,但在基于PaO/FiO的严重程度组中保持相似。
基于氧合障碍的ARDS严重程度不能反映VILI的先决条件和决定因素。这应促使人们重新考虑基于氧合障碍而非VILI决定因素来推荐呼吸支持。