Yutaka Yojiro, Nishikawa Shigeto, Tanaka Satona, Ohsumi Akihiro, Nakajima Daisuke, Menju Toshi, Hidaka Yu, Kato Takao, Date Hiroshi
Department of Thoracic Surgery, Kyoto University Graduate School of Medicine, Kyoto, Japan.
Department of Biomedical Statistics and Bioinformatics, Kyoto University, Kyoto, Japan.
JTCVS Tech. 2024 Sep 11;28:141-150. doi: 10.1016/j.xjtc.2024.08.027. eCollection 2024 Dec.
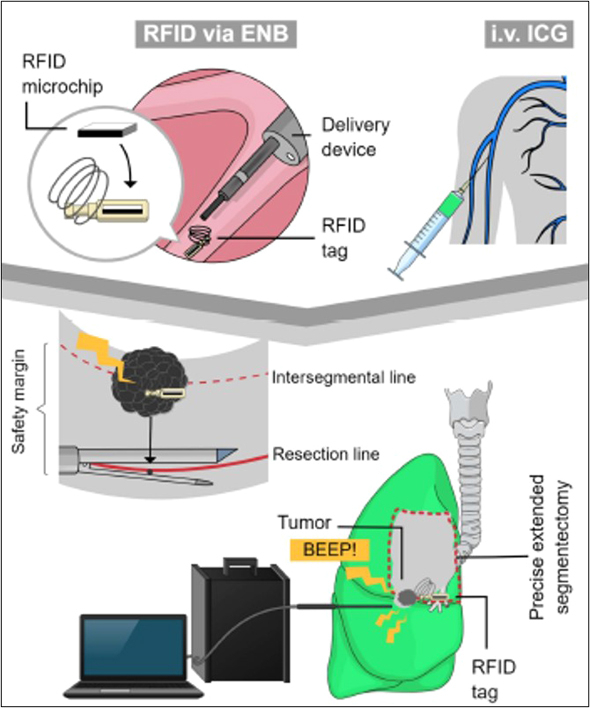
We developed a technique to determine deep surgical margins using radiofrequency identification markers. This study assessed the feasibility of this technique during extended segmentectomy of intersegmental lesions.
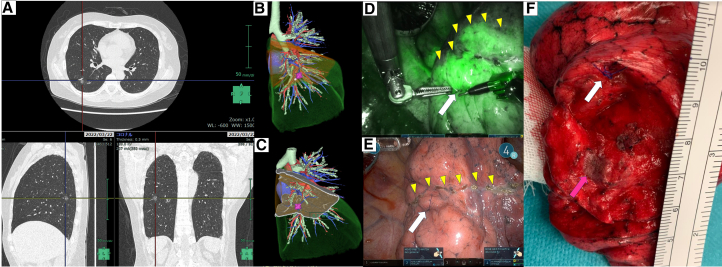
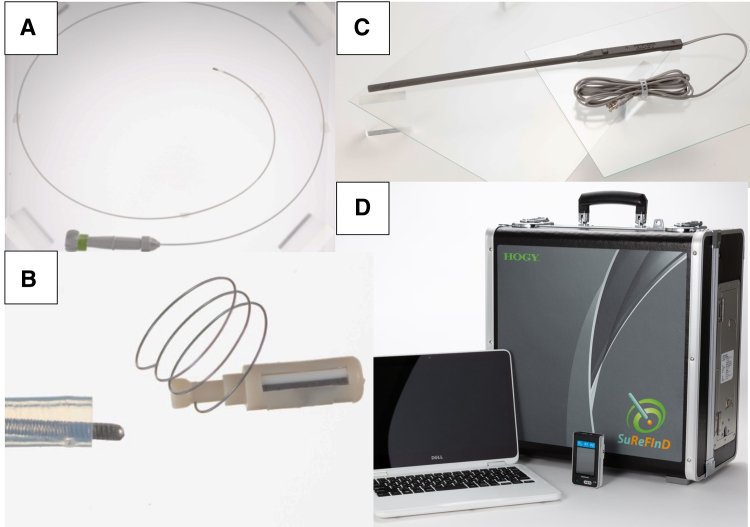
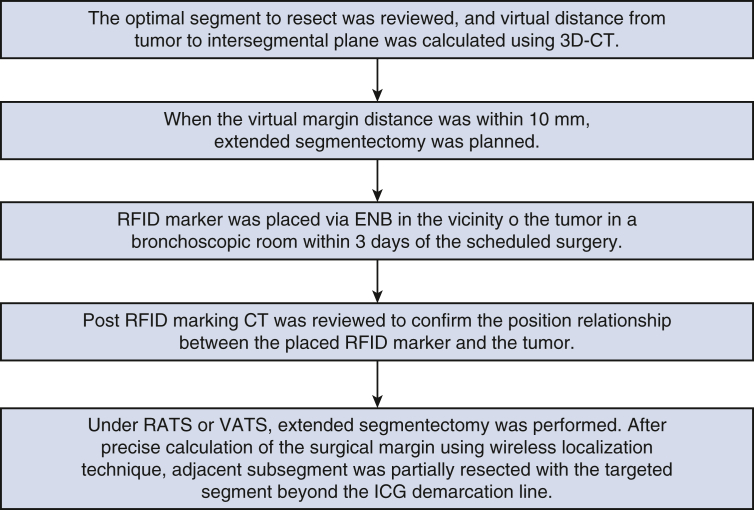
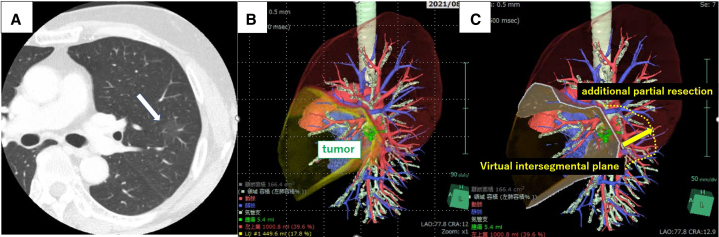
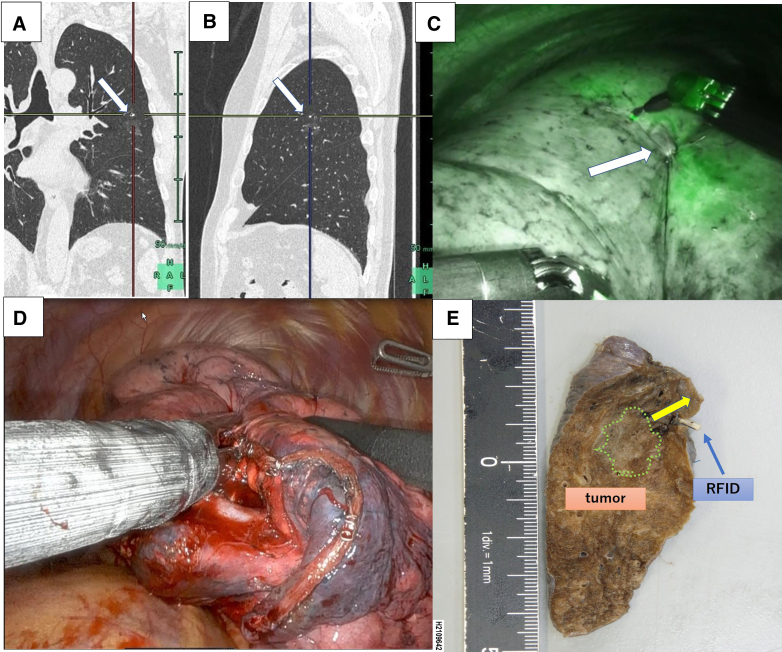
A single-center, prospective, single-arm study was performed from 2020 to 2023. Small pulmonary lesions suspicious for malignancy locating the virtual intersegmental plane based on 3-dimensional imagery were included. Markers were placed in the vicinity of the lesions using electromagnetic navigation bronchoscopy. In addition to indocyanine green injection, surgeons used wireless signal strength to determine the best resection line without lung palpation to obtain surgical margins of 10 mm or the same size as the tumor.
We analyzed 75 lesions in 75 patients. Median lesion size and depth from the pleura were 12.0 mm and 23.6 mm, respectively. Three-dimensional imagery identified lesions at a median distance of 7.0 mm from the virtual intersegmental plane. The median marker-lesion and marker-virtual intersegmental plane distances were 5.8 mm and 4.9 mm, respectively. Complex segmentectomy was performed in 64 of 75 patients (85.3%). The indocyanine green and preoperative simulated intersegmental lines agreed in 92.0% (69/75). In 6 cases (8.0%), the resection line was determined using radiofrequency identification markers to obtain adequate margins because the indocyanine green undyed area was smaller than the preoperatively simulated one. In 1 patient, planned segmentectomy was converted to lobectomy because of a misplaced radiofrequency identification marker (1.3%). The successful tumor resection rate was 98.7%. The median surgical margin was 16.0 mm.
Use of radiofrequency identification markers enabled precise extended segmentectomy with adequate surgical margins.
我们开发了一种使用射频识别标记来确定深部手术切缘的技术。本研究评估了该技术在节段间病变扩大切除术期间的可行性。
2020年至2023年进行了一项单中心、前瞻性、单臂研究。纳入基于三维成像定位在虚拟节段间平面的可疑恶性小肺病变。使用电磁导航支气管镜在病变附近放置标记。除了注射吲哚菁绿外,外科医生还使用无线信号强度来确定最佳切除线,无需触诊肺组织,以获得10毫米或与肿瘤大小相同的手术切缘。
我们分析了75例患者的75个病变。病变的中位大小和距胸膜的深度分别为12.0毫米和23.6毫米。三维成像显示病变距虚拟节段间平面的中位距离为7.0毫米。标记与病变以及标记与虚拟节段间平面的中位距离分别为5.8毫米和4.9毫米。75例患者中有64例(85.3%)进行了复杂节段切除术。吲哚菁绿与术前模拟的节段间线相符的比例为92.0%(69/75)。在6例(8.0%)病例中,由于吲哚菁绿未染色区域小于术前模拟区域,使用射频识别标记确定切除线以获得足够的切缘。在1例患者中,由于射频识别标记放置错误,计划的节段切除术改为肺叶切除术(1.3%)。肿瘤成功切除率为98.7%。中位手术切缘为16.0毫米。
使用射频识别标记能够实现精确的扩大节段切除术,并获得足够的手术切缘。