Khendek Leticia, Castro-Rojas Cyd, Nelson Constance, Alquraish Mosab, Karns Rebekah, Kasten Jennifer, Teng Xiao, Miethke Alexander G, Taylor Amy E
Department of Pediatrics, Division of Gastroenterology, Hepatology, and Nutrition, Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio, USA.
Center for Autoimmune Liver Disease (CALD), Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio, USA.
Hepatol Commun. 2024 Dec 11;9(1). doi: 10.1097/HC9.0000000000000594. eCollection 2025 Jan 1.
Children with autoimmune liver disease (AILD) may develop fibrosis-related complications necessitating a liver transplant. We hypothesize that tissue-based analysis of liver fibrosis by second harmonic generation (SHG) microscopy with artificial intelligence analysis can yield prognostic biomarkers in AILD.
Patients from single-center studies with unstained slides from clinically obtained liver biopsies at AILD diagnosis were identified. Baseline demographics and liver biochemistries at diagnosis and 1 year were collected. Clinical endpoints studied included the presence of varices, variceal bleeding, ascites, HE, and liver transplant. In collaboration with HistoIndex, unstained slides underwent SHG/artificial intelligence analysis to map fibrosis according to 10 quantitative fibrosis parameters based on tissue location, including total, periportal, perisinusoidal, and pericentral area and length of strings.
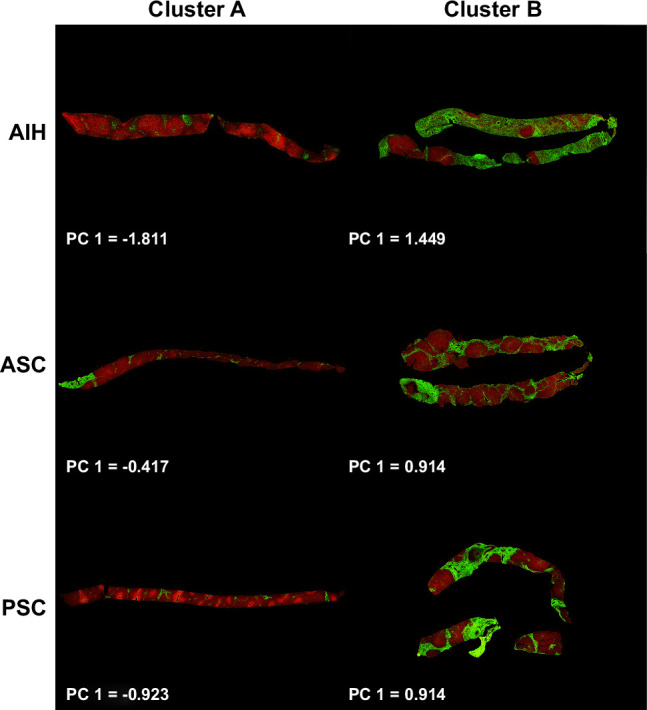
Sixty-three patients with AIH (51%), primary sclerosing cholangitis (30%), or autoimmune sclerosing cholangitis (19%) at a median of 14 years old (range: 3-24) were included. An unsupervised analysis of quantitative fibrosis parameters representing total and portal fibrosis identified a patient cluster with more primary sclerosing cholangitis/autoimmune sclerosing cholangitis. This group had more fibrosis at diagnosis by METAVIR classification of histopathological review of biopsies (2.5 vs. 2; p = 0.006). This quantitative fibrosis pattern also predicted abnormal 12-month ALT with an OR of 3.6 (1.3-10, p = 0.014), liver complications with an HR of 3.2 (1.3-7.9, p = 0.01), and liver transplantation with an HR of 20.1 (3-135.7, p = 0.002).
The application of SHG/artificial intelligence algorithms in pediatric-onset AILD provides improved insight into liver histopathology through fibrosis mapping. SHG allows objective identification of patients with biliary tract involvement, which may be associated with a higher risk for refractory disease.
自身免疫性肝病(AILD)患儿可能会出现与纤维化相关的并发症,从而需要进行肝移植。我们假设,通过二次谐波产生(SHG)显微镜结合人工智能分析对肝纤维化进行组织学分析,能够在AILD中产生预后生物标志物。
从单中心研究中识别出在AILD诊断时具有临床获取的肝活检未染色玻片的患者。收集诊断时和1年时的基线人口统计学数据及肝脏生化指标。研究的临床终点包括静脉曲张的存在、静脉曲张出血、腹水、肝性脑病(HE)和肝移植。与HistoIndex合作,对未染色玻片进行SHG/人工智能分析,根据基于组织位置的10个定量纤维化参数绘制纤维化图谱,这些参数包括总量、汇管区周围、窦周和中央静脉周围区域以及条索长度。
纳入了63例年龄中位数为14岁(范围:3 - 24岁)的自身免疫性肝炎(AIH)(51%)、原发性硬化性胆管炎(30%)或自身免疫性硬化性胆管炎(19%)患者。对代表总量和门脉纤维化的定量纤维化参数进行无监督分析,识别出一个原发性硬化性胆管炎/自身免疫性硬化性胆管炎更多的患者集群。通过活检组织病理学复查的METAVIR分类,该组在诊断时纤维化程度更高(2.5对2;p = 0.006)。这种定量纤维化模式还预测12个月时ALT异常的比值比为3.6(1.3 - 10,p = 0.014),发生肝脏并发症的风险比为3.2(1.3 - 7.9,p = 0.01),肝移植的风险比为20.1(3 - 135.7,p = 0.002)。
SHG/人工智能算法在儿童期AILD中的应用通过纤维化图谱绘制,能更深入地了解肝脏组织病理学。SHG能够客观识别出胆道受累患者,这可能与难治性疾病的较高风险相关。