Coppolino Francesco, Brunetti Simona, Bottazzo Leonardo Maria, Cosenza Gianluigi, Sansone Pasquale, Fiore Marco, Passavanti Maria Beatrice, Pota Vincenzo, Pace Maria Caterina
Department of Women, Children and General and Specialized Surgery, University of Campania Luigi Vanvitelli, Naples, Italy.
Local Reg Anesth. 2024 Dec 11;17:99-105. doi: 10.2147/LRA.S487981. eCollection 2024.
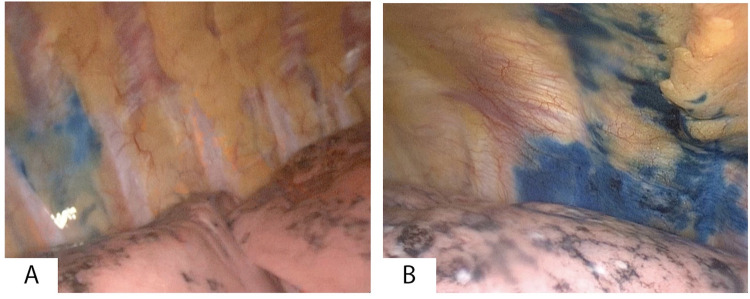
Thoracic surgery often results in severe chronic postoperative pain. Current evidence favors two locoregional techniques. Thoracic Epidural Anesthesia (TEA), the gold standard, and Thoracic Paravertebral Block (TPVB), which is associated with fewer side effects but is limited by short duration of action of local anesthetics (LA) and potential failure due to improper drug distribution. This study investigates the use of dexmedetomidine (DEX) as adjuvant to prolong the effects of LA in TPVB, with methylene blue used for visual confirmation of accurate injectate spread.
We observed 6 patients undergoing Video-Assisted Thoracoscopy (VATS) lobectomy who received TPVB with ropivacaine, DEX and methylene blue. The primary endpoint was postoperative pain recorded at 1, 12, 24, 48 hours using Numeric Rating Scale (NRS); the secondary endpoints were cumulative opioid consumption in the first 24 hours in Milligram Morphine Equivalents (MME); adverse events: occurrence of bradycardia, hypotension, Postoperative Nausea and Vomiting (PONV); length of hospital stay. All patients completed the study.
Our results showed optimal pain scores, with NRS scores always below 4, decreased need for opioids, and prolonged analgesia. None of the patients had bradycardia nor PONV, but two patients experienced acute and self-limited hypotension following TPVB.
Thoracic Paravertebral Block with Dexmedetomidine and methylene blue was effective and safe in controlling postoperative pain. Methylene blue could help improving knowledge on anesthetics distribution to reduce failure rates.
胸外科手术常常导致严重的慢性术后疼痛。目前的证据支持两种局部区域技术。胸段硬膜外麻醉(TEA)是金标准,而胸段椎旁阻滞(TPVB)副作用较少,但受局部麻醉药(LA)作用时间短以及药物分布不当可能导致失败的限制。本研究调查右美托咪定(DEX)作为佐剂用于延长LA在TPVB中的作用效果,使用亚甲蓝来视觉确认注射剂的准确扩散。
我们观察了6例接受电视辅助胸腔镜(VATS)肺叶切除术的患者,他们接受了罗哌卡因、DEX和亚甲蓝的TPVB。主要终点是使用数字评分量表(NRS)在术后1、12、24、48小时记录的疼痛情况;次要终点是前24小时以毫克吗啡当量(MME)计算的累积阿片类药物消耗量;不良事件:心动过缓、低血压、术后恶心呕吐(PONV)的发生情况;住院时间。所有患者均完成了研究。
我们的结果显示疼痛评分最佳,NRS评分始终低于4,阿片类药物需求减少,镇痛时间延长。没有患者出现心动过缓或PONV,但有2例患者在TPVB后出现急性且自限性的低血压。
右美托咪定联合亚甲蓝的胸段椎旁阻滞在控制术后疼痛方面有效且安全。亚甲蓝有助于提高对麻醉药分布的了解以降低失败率。