Xu Yang, Li Xiao-Kun, Zhou Hai, Cong Zhuang-Zhuang, Wu Wen-Jie, Qiang Yong, Shen Yi
Department of Cardiothoracic Surgery, Jingling Hospital, Jingling School of Clinical Medicine, Nanjing Medical University, Nanjing, China.
Department of Cardiothoracic Surgery, Jingling Hospital, School of Medicine, Southeast University, Nanjing, China.
J Thorac Dis. 2020 Aug;12(8):4115-4125. doi: 10.21037/jtd-20-1068B.
Paravertebral block (PVB) conducted by epidural catheter is a prevalent pain management for patients undergoing video-assisted thoracoscopic surgery (VATS) lobectomy. The aim of this study was to assess the efficacy and safety of paravertebral block with a modified PVB (MPVB) catheter under surgeon's direct vision after video-assisted thoracoscopic lobectomy.
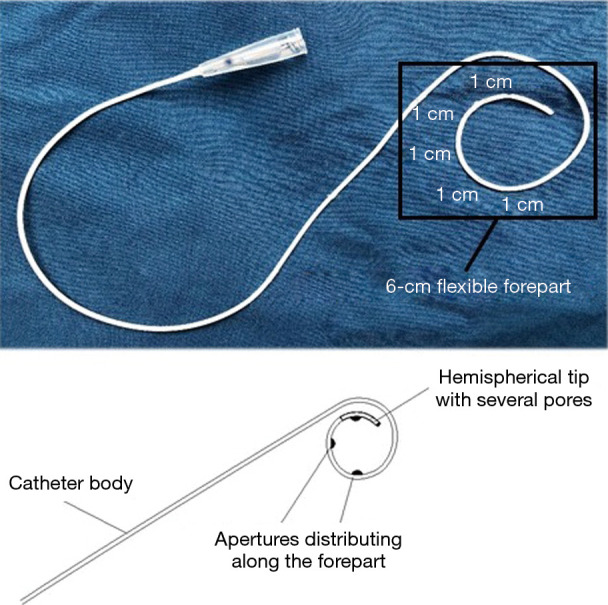
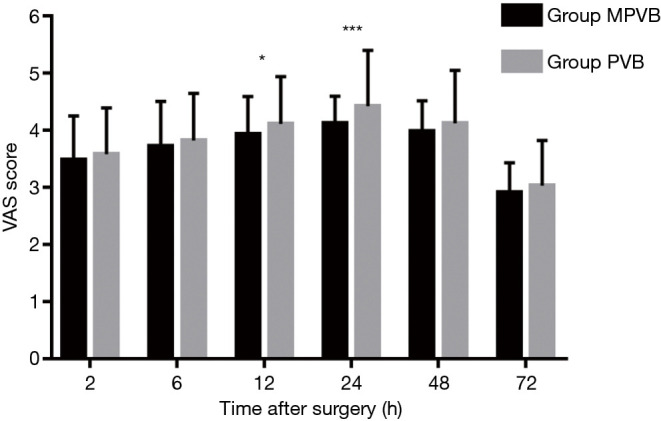
Three hundred fifty-six patients undergoing VATS lobectomy were retrospectively reviewed and divided into two groups consecutively according to the catheter applied in PVB procedure (PVB group and MPVB group). In the MPVB group, a modified catheter with a flexible forepart and more apertures distributing along the forepart than the conventional epidural catheter was introduced. An infusion pump containing of 150 mL mixture was connected to the catheter to provide sustained regional analgesia. Intramuscular dezocine 10 mg was administered as a rescue medication when necessary. Postoperative pain management effect was assessed by visual analog scale (VAS) at rest and on coughing. Spirometry values and blood gas analysis were monitored and recorded for the first 3 postoperative days (PODs). Analgesia-related adverse events, characteristics of PVB procedure and postoperative major complication were also compared between the two groups.
There were 172 patients who received PVB with conventional epidural catheter in the PVB group, and 184 patients were performed PVB with modified paravertebral catheter in the MPVB group. Significantly lower pain score at rest was found in MPVB group at 24 h postoperatively (P=0.006). The pain score on coughing in MPVB group was significantly lower than that in PVB group at 12 and 24 h postoperatively (P=0.037 and P<0.001, respectively). Patients needing for rescue medication was significantly lower in the MPVB group (P=0.028). The incidence of pleural perforation was lower in the MPVB group (P=0.020). Postoperative spirometry values revealed comparable pulmonary function between the two groups, and arterial blood gas analysis showed a normal range of pH and PaCO2 in both groups. There was no significant difference of analgesia-related adverse events as well as major complications between the two groups.
PVB with modified catheter under surgeon's direct vision was effective and safe after video-assisted thoracoscopic lobectomy.
通过硬膜外导管进行的椎旁阻滞(PVB)是电视辅助胸腔镜手术(VATS)肺叶切除术患者常用的疼痛管理方法。本研究的目的是评估电视辅助胸腔镜肺叶切除术后在外科医生直视下使用改良PVB(MPVB)导管进行椎旁阻滞的有效性和安全性。
回顾性分析356例行VATS肺叶切除术的患者,并根据PVB操作中使用的导管将其连续分为两组(PVB组和MPVB组)。在MPVB组中,引入了一种改良导管,其前端灵活,且沿前端分布的孔比传统硬膜外导管更多。将一个装有150 mL混合液的输液泵连接到导管上,以提供持续的区域镇痛。必要时给予肌肉注射地佐辛10 mg作为补救药物。术后通过静息和咳嗽时的视觉模拟量表(VAS)评估疼痛管理效果。在术后第1至3天(POD)监测并记录肺活量测定值和血气分析结果。还比较了两组之间镇痛相关不良事件、PVB操作特点和术后主要并发症。
PVB组有172例患者接受了传统硬膜外导管的PVB,MPVB组有184例患者接受了改良椎旁导管的PVB。MPVB组术后24小时静息时疼痛评分显著更低(P = 0.006)。MPVB组术后12小时和24小时咳嗽时的疼痛评分显著低于PVB组(分别为P = 0.037和P < 0.001)。MPVB组需要补救药物的患者显著更少(P = 0.028)。MPVB组胸膜穿孔的发生率更低(P = 0.020)。术后肺活量测定值显示两组肺功能相当,动脉血气分析显示两组pH和PaCO2均在正常范围内。两组之间镇痛相关不良事件以及主要并发症无显著差异。
电视辅助胸腔镜肺叶切除术后在外科医生直视下使用改良导管进行PVB是有效且安全的。