Al Qureshah Fahd, Le Pen Jérémie, de Weerd Nicole A, Moncada-Velez Marcela, Materna Marie, Lin Daniel C, Milisavljevic Baptiste, Vianna Fernanda, Bizien Lucy, Lorenzo Lazaro, Lecuit Marc, Pommier Jean-David, Keles Sevgi, Ozcelik Tayfun, Pedraza-Sanchez Sigifredo, de Prost Nicolas, El Zein Loubna, Hammoud Hassan, Ng Lisa F P, Halwani Rabih, Saheb Sharif-Askari Narjes, Lau Yu Lung, Tam Anthony R, Singh Neha, Bhattad Sagar, Berkun Yackov, Chantratita Wasun, Aguilar-López Raúl, Shahrooei Mohammad, Abel Laurent, Bastard Paul, Jouanguy Emmanuelle, Béziat Vivien, Zhang Peng, Rice Charles M, Cobat Aurélie, Zhang Shen-Ying, Hertzog Paul J, Casanova Jean-Laurent, Zhang Qian
St Giles Laboratory of Human Genetics of Infectious Diseases, Rockefeller Branch, Rockefeller University, New York, NY, USA.
Wellness and Preventive Medicine Institute, King Abdulaziz City for Science and Technology , Riyadh, Saudi Arabia.
J Exp Med. 2025 Feb 3;222(2). doi: 10.1084/jem.20241413. Epub 2024 Dec 16.
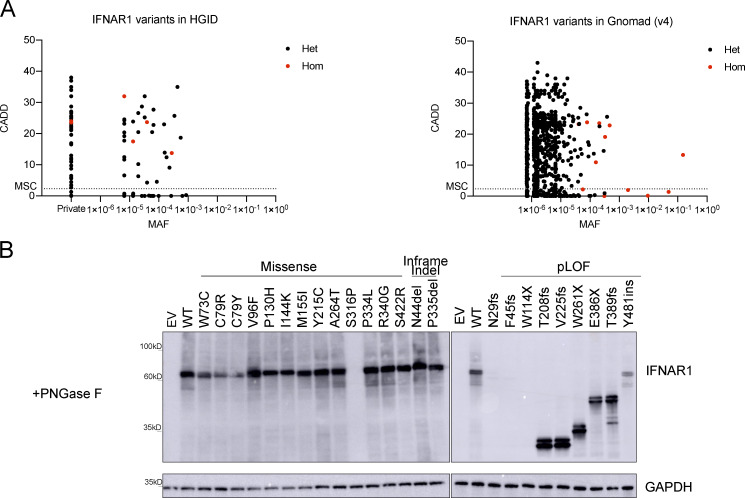
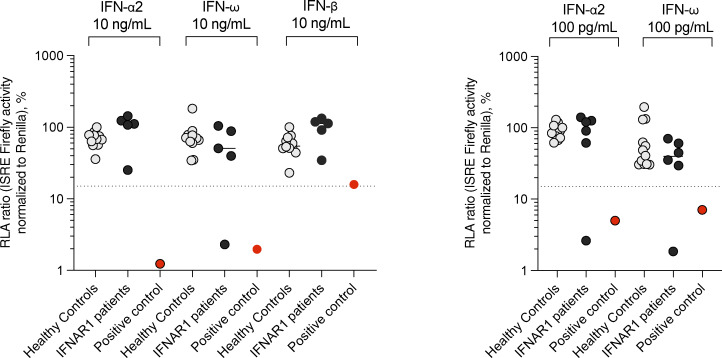
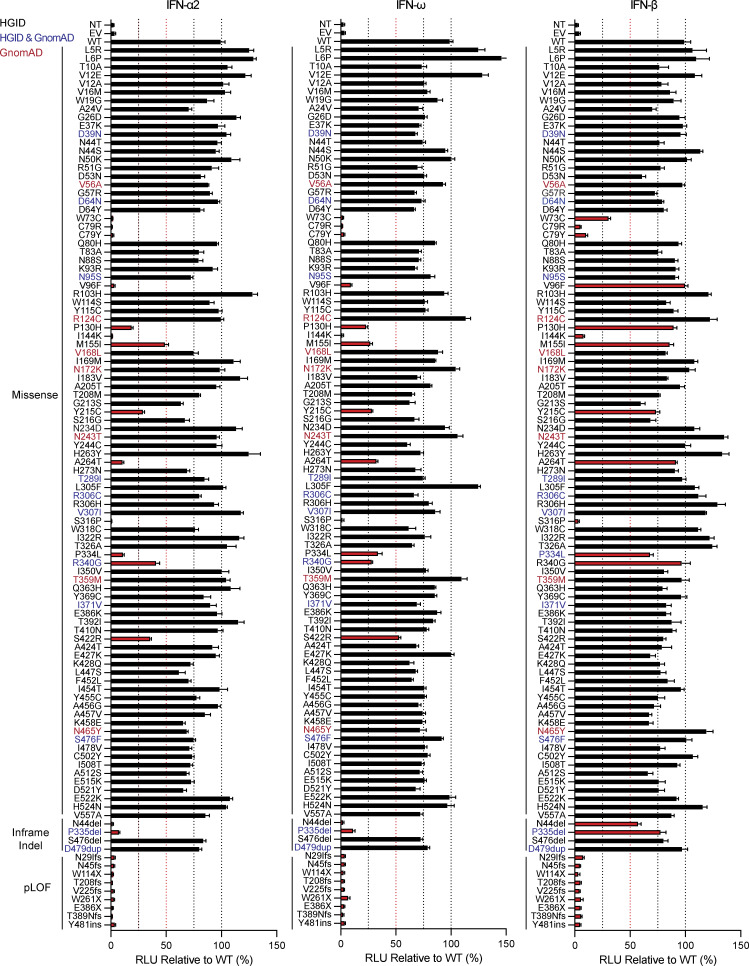
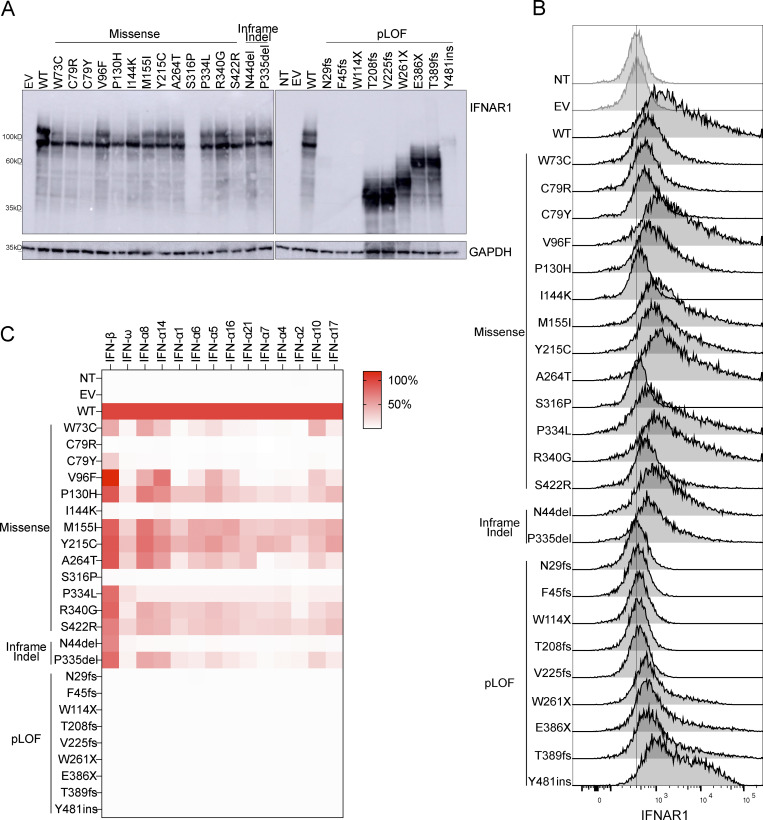
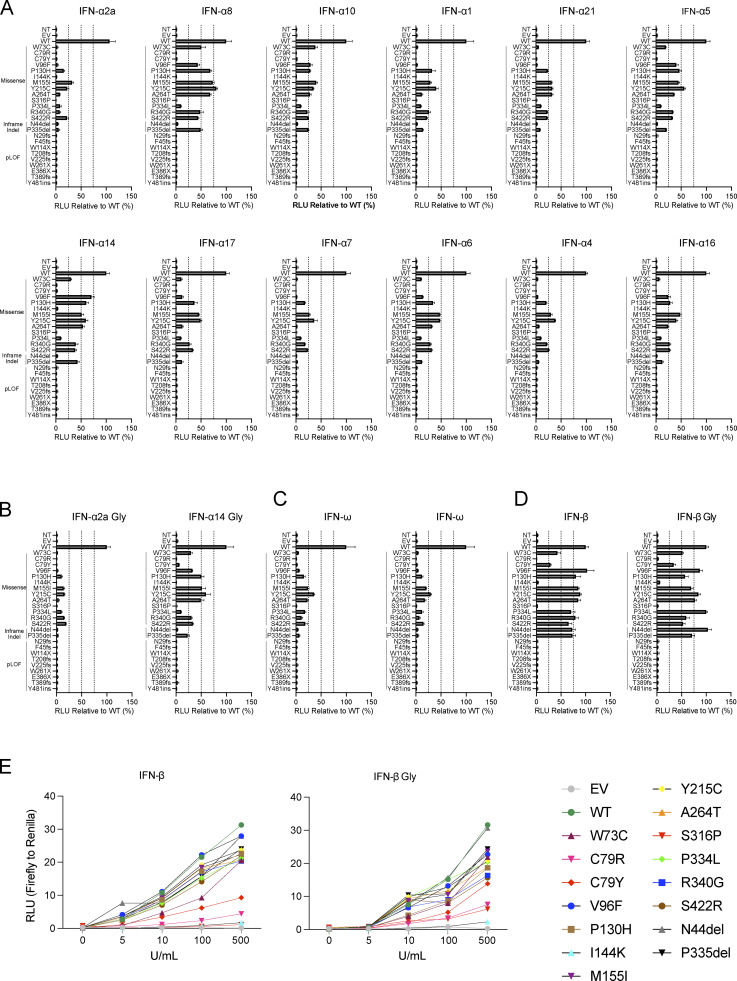
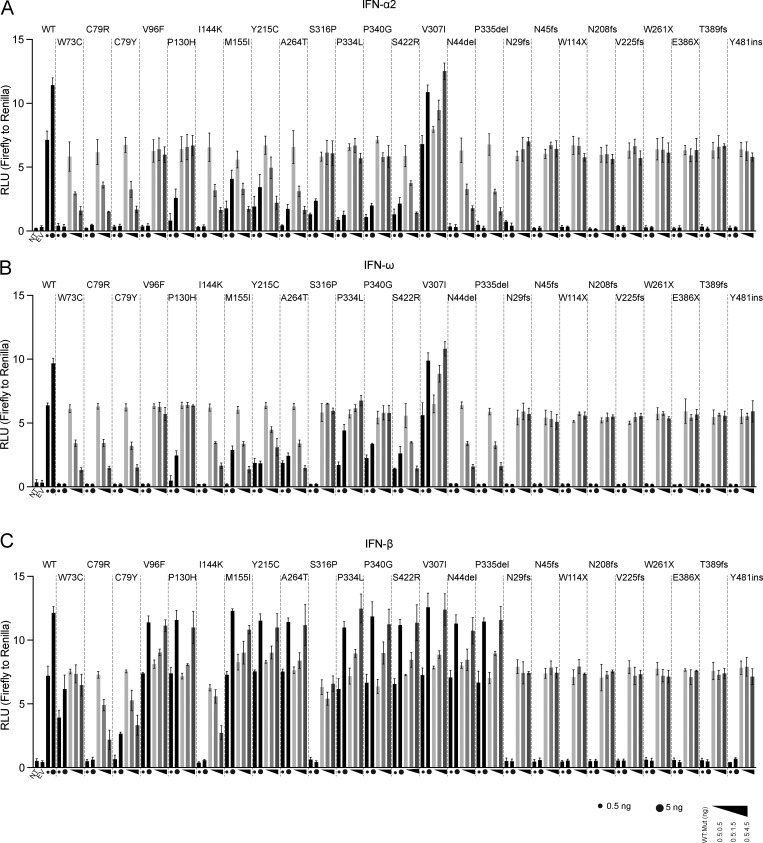
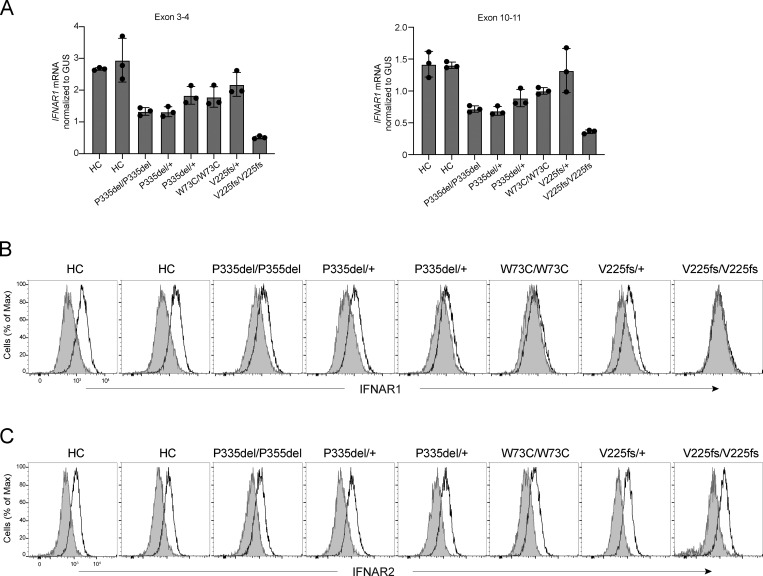
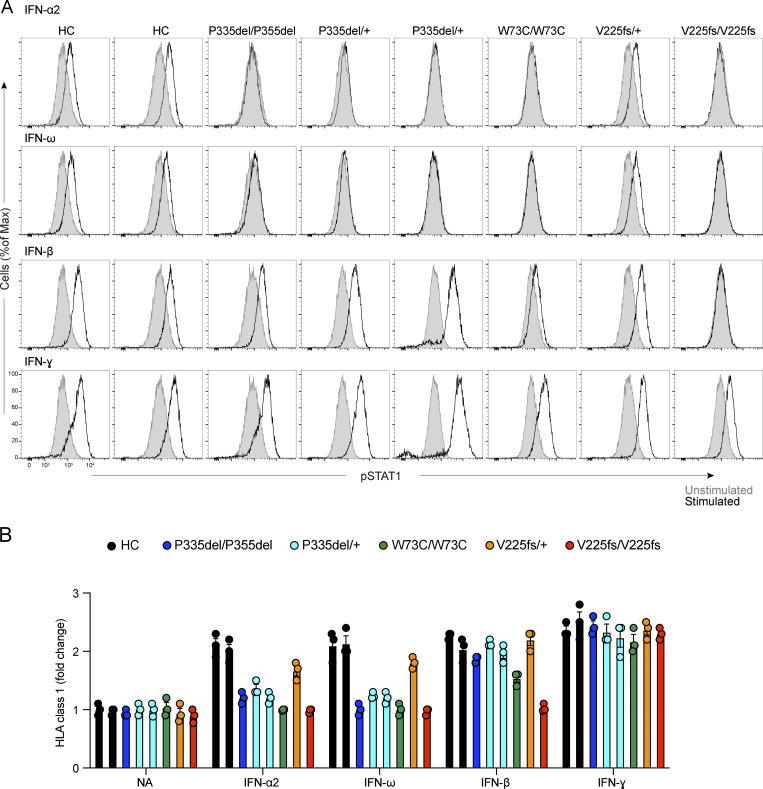
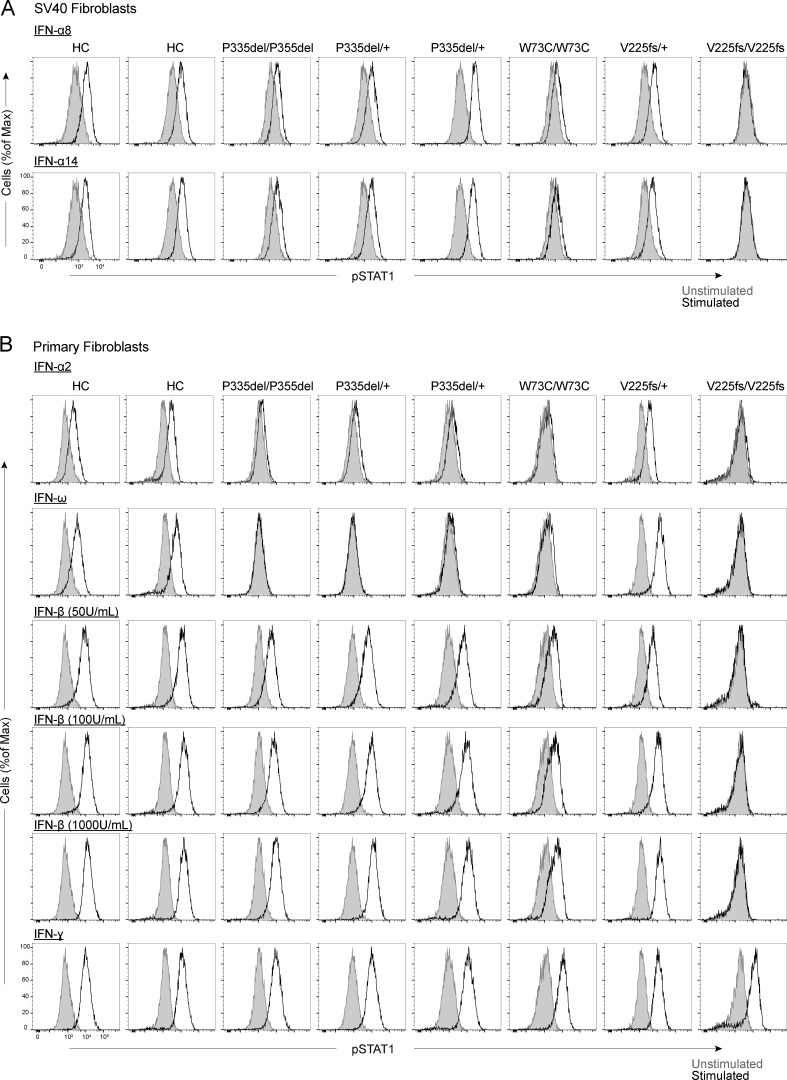
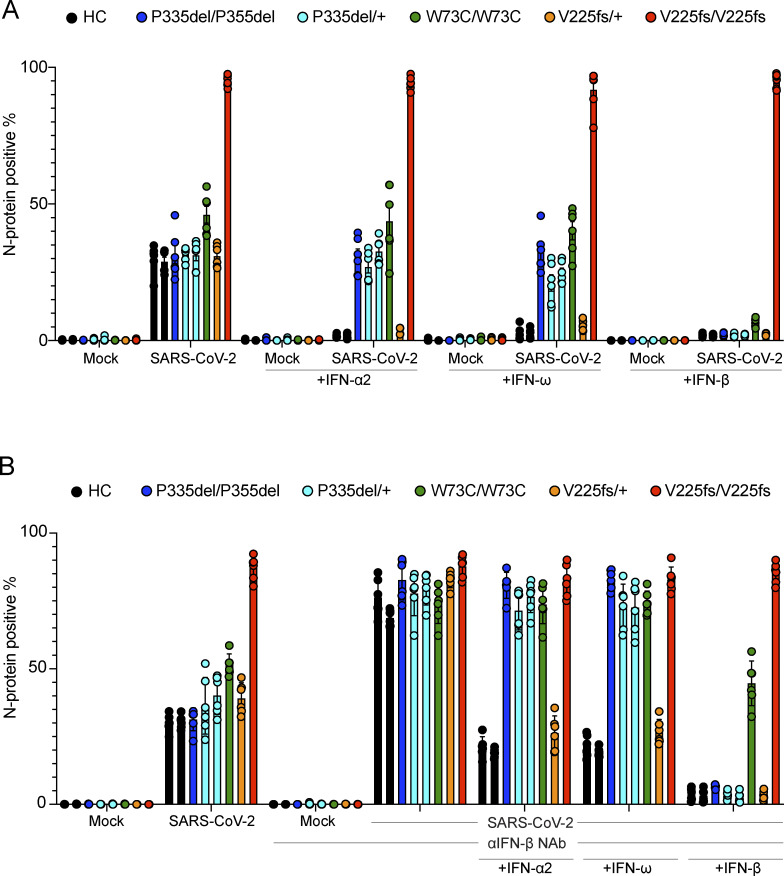
Autosomal recessive deficiency of the IFNAR1 or IFNAR2 chain of the human type I IFN receptor abolishes cellular responses to IFN-α, -β, and -ω, underlies severe viral diseases, and is globally very rare, except for IFNAR1 and IFNAR2 deficiency in Western Polynesia and the Arctic, respectively. We report 11 human IFNAR1 alleles, the products of which impair but do not abolish responses to IFN-α and -ω without affecting responses to IFN-β. Ten of these alleles are rare in all populations studied, but the remaining allele (P335del) is common in Southern China (minor allele frequency ≈2%). Cells heterozygous for these variants display a dominant phenotype in vitro with impaired responses to IFN-α and -ω, but not -β, and viral susceptibility. Negative dominance, rather than haploinsufficiency, accounts for this dominance. Patients heterozygous for these variants are prone to viral diseases, attesting to both the dominance of these variants clinically and the importance of IFN-α and -ω for protective immunity against some viruses.
人类I型干扰素受体的IFNAR1或IFNAR2链的常染色体隐性缺陷会消除细胞对IFN-α、-β和-ω的反应,是严重病毒性疾病的基础,并且在全球范围内非常罕见,西波利尼西亚和北极地区分别存在IFNAR1和IFNAR2缺陷的情况除外。我们报告了11个人类IFNAR1等位基因,其产物会损害但不会消除对IFN-α和-ω的反应,同时不影响对IFN-β的反应。在所有研究的人群中,这些等位基因中有10个很罕见,但其余等位基因(P335del)在中国南方很常见(次要等位基因频率约为2%)。这些变体的杂合细胞在体外表现出显性表型,对IFN-α和-ω的反应受损,但对IFN-β的反应不受影响,且具有病毒易感性。这种显性现象是由负显性而非单倍体不足导致的。这些变体的杂合患者易患病毒性疾病,这证明了这些变体在临床上的显性以及IFN-α和-ω对某些病毒的保护性免疫的重要性。