Bsteh Gabriel, Hegen Harald, Krajnc Nik, Föttinger Fabian, Altmann Patrick, Auer Michael, Berek Klaus, Kornek Barbara, Leutmezer Fritz, Macher Stefan, Monschein Tobias, Ponleitner Markus, Rommer Paulus, Schmied Christiane, Zebenholzer Karin, Zulehner Gudrun, Zrzavy Tobias, Deisenhammer Florian, Di Pauli Franziska, Pemp Berthold, Berger Thomas
Department of Neurology, Medical University of Vienna, Vienna, Austria.
Comprehensive Center for Clinical Neurosciences and Mental Health, Medical University of Vienna, Vienna, Austria.
Ann Clin Transl Neurol. 2025 Feb;12(2):345-354. doi: 10.1002/acn3.52279. Epub 2024 Dec 16.
To investigate retinal layer thinning as a biomarker of disease-modifying treatment (DMT) effects in relapsing multiple sclerosis (RMS).
From an ongoing prospective observational study, we included patients with RMS, who (i) had an optical coherence tomography (OCT) scan within 6 to 12 months after DMT start (rebaseline) and ≥1 follow-up OCT ≥12 months after rebaseline and (ii) adhered to DMT during follow-up. Differences between DMT in thinning of peripapillary-retinal-nerve-fiber-layer (pRNFL) and macular ganglion cell-plus-inner plexiform-layer (GCIPL) were analyzed using mixed-effects linear regression. Eyes suffering optic neuritis during follow-up were excluded.
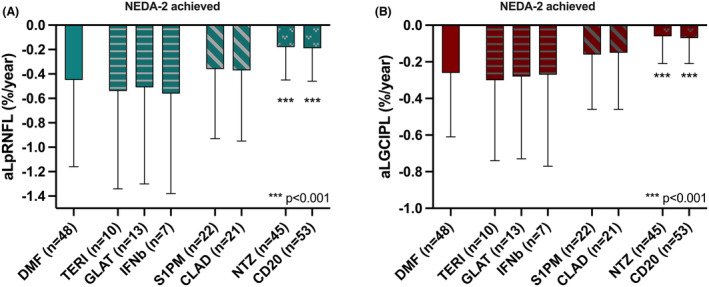
We included 291 RMS patients (mean age 30.8 years [SD 7.9], 72.9% female, median disease duration 9 months [range 6-94], median rebaseline-to-last-follow-up-interval 32 months [12-82]). Mean annualized rates of retinal layer thinning (%/year) in reference to DMF (n = 84, GCIPL 0.28, pRNFL 0.53) were similar under TERI (n = 18, GCIPL 0.34, pRNFL 0.59), GLAT (n = 24, GCIPL 0.32, pRNFL 0.56), and IFNb (n = 13, GCIPL 0.33, pRNFL 0.60) were slightly lower under S1PM (n = 27, GCIPL 0.19, pRNFL 0.42) and CLA (n = 23, GCIPL 0.20, pRNFL 0.42), and were significantly lower under NTZ (n = 47, GCIPL 0.09, pRNFL 0.24; both p < 0.001) and antiCD20 (n = 55, GCIPL 0.10, pRNFL 0.23; both p < 0.001). In patients achieving NEDA-2, observed thinning rates were lower overall, but still significantly lower under NTZ and antiCD20.
Applying a rebaselining concept, retinal layer thinning differentiates DMT effects even in clinically stable patients and, thus, might be a useful biomarker to monitor DMT efficacy on subclinical neuroaxonal degeneration-at least on a group level.
研究视网膜层变薄作为复发型多发性硬化症(RMS)疾病修饰治疗(DMT)效果生物标志物的情况。
在一项正在进行的前瞻性观察研究中,我们纳入了RMS患者,这些患者(i)在开始DMT治疗后6至12个月内进行了光学相干断层扫描(OCT)(重新基线),且在重新基线后≥12个月进行了≥1次随访OCT,并且(ii)在随访期间坚持DMT治疗。使用混合效应线性回归分析DMT在视乳头周围视网膜神经纤维层(pRNFL)和黄斑神经节细胞加内丛状层(GCIPL)变薄方面的差异。排除随访期间患视神经炎的眼睛。
我们纳入了291例RMS患者(平均年龄30.8岁[标准差7.9],72.9%为女性,疾病持续时间中位数9个月[范围6 - 94],重新基线至最后一次随访间隔中位数32个月[12 - 82])。相对于二甲基富马酸盐(DMF)(n = 84,GCIPL 0.28,pRNFL 0.53),在替利氟胺(TERI)(n = 18,GCIPL 0.34,pRNFL 0.59)、格拉替雷(GLAT)(n = 24,GCIPL 0.32,pRNFL 0.56)和干扰素β(IFNb)(n = 13,GCIPL 0.33,pRNFL 0.60)治疗下,视网膜层变薄的年均速率(%/年)相似;在西尼莫德(S1PM)(n = 27,GCIPL 0.19,pRNFL 0.42)和克拉屈滨(CLA)(n = 23,GCIPL 0.20,pRNFL 0.42)治疗下稍低;在那他珠单抗(NTZ)(n = 47,GCIPL 0.09,pRNFL 0.24;两者p < 0.001)和抗CD20(n = 55,GCIPL 0.10,pRNFL 0.23;两者p < 0.001)治疗下显著更低。在达到无疾病活动状态2(NEDA -2)的患者中,观察到的变薄速率总体较低,但在NTZ和抗CD20治疗下仍显著更低。
应用重新基线概念,即使在临床稳定的患者中,视网膜层变薄也能区分DMT的效果,因此,它可能是监测DMT对亚临床神经轴突退变疗效的有用生物标志物——至少在群体水平上是如此。