Department of Neurology, Medical University of Vienna, Vienna, Austria.
Department of Neurology, Medical University of Innsbruck, Innsbruck, Austria.
Eur J Neurol. 2021 Jun;28(6):2037-2045. doi: 10.1111/ene.14829. Epub 2021 Apr 2.
Peripapillary retinal nerve fiber layer (pRNFL) and macular ganglion cell plus inner plexiform layer (GCIPL) thinning are markers of neuroaxonal degeneration in multiple sclerosis (MS), which is reduced by disease-modifying treatment (DMT). We aimed to investigate the potential of pRNFL and GCIPL thinning for prediction of DMT failure in relapsing MS (RMS).
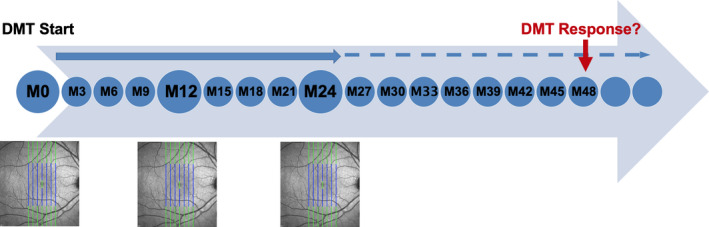
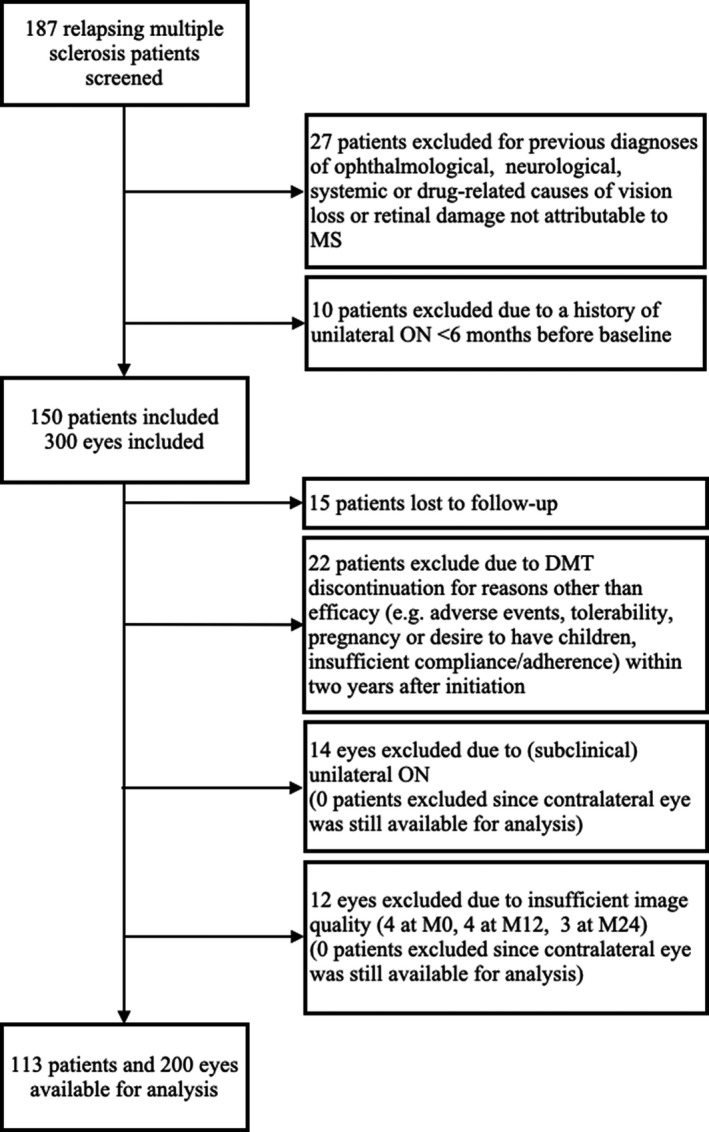
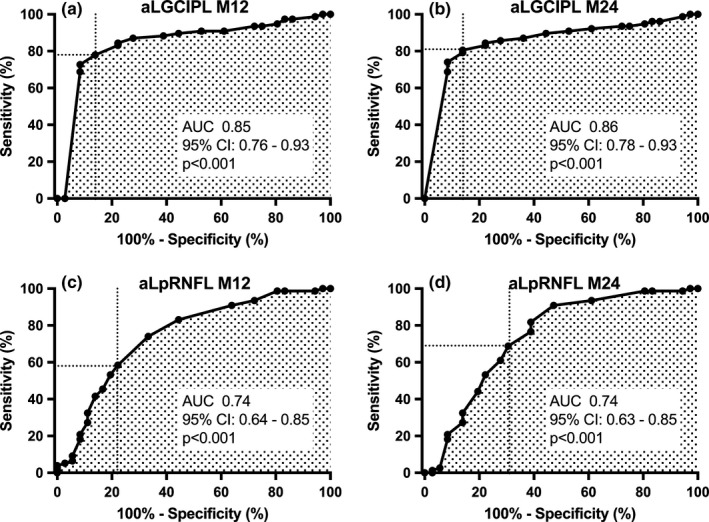
In this 4-year prospective observational study on 113 RMS patients, pRNFL and GCIPL were measured at DMT initiation and after 12 months (M12) and 24 months (M24). Treatment failure was defined as 6-month confirmed Expanded Disability Status Scale (EDSS) progression and/or Symbol Digit Modalities Test (SDMT) worsening. Optimal cutoff values for predicting treatment failure were determined by receiver operating characteristic analyses and hazard ratios (HRs) by multivariable Cox regression adjusting for age, sex, disease duration, EDSS/SDMT, and DMT class.
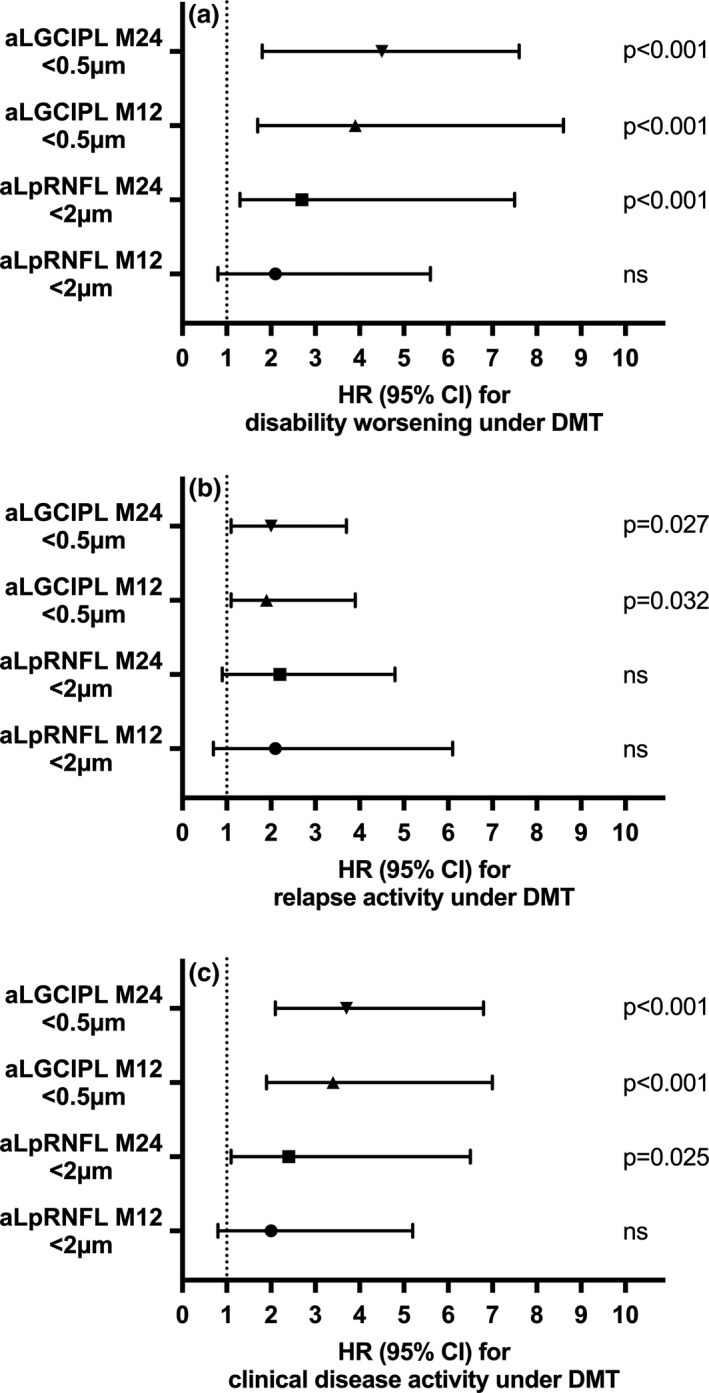
Thinning of GCIPL >0.5 μm/year at M24 showed superior value for treatment failure prediction (HR: 4.5, 95% confidence interval [CI]: 1.8-7.6, p < 0.001; specificity 91%, sensitivity 81%), followed by GCIPL >0.5 μm at M12 (odds ratio [OR]: 3.9, 95% CI: 1.4-6.9, p < 0.001; specificity 85%, sensitivity 78%), and pRNFL ≥2 μm/year at M24 (OR: 3.7, 95% CI: 1.1-6.5, p = 0.023; specificity 84%, sensitivity 69%), whereas pRNFL at M12 was not predictive.
GCIPL, and to a lesser degree pRNFL, thinning predicts disability progression after DMT initiation and may be a useful and accessible biomarker of treatment failure in RMS.
视盘周围视网膜神经纤维层(pRNFL)和黄斑神经节细胞加内丛状层(GCIPL)变薄是多发性硬化症(MS)神经轴突变性的标志物,这种变性可被疾病修正治疗(DMT)所减轻。我们旨在研究 pRNFL 和 GCIPL 变薄对预测复发型多发性硬化症(RMS)DMT 失败的潜在价值。
在这项针对 113 例 RMS 患者的 4 年前瞻性观察性研究中,在 DMT 起始时以及 12 个月(M12)和 24 个月(M24)时测量了 pRNFL 和 GCIPL。将 6 个月确认的扩展残疾状况量表(EDSS)进展和/或符号数字模态测试(SDMT)恶化定义为治疗失败。通过接受者操作特征分析确定预测治疗失败的最佳截断值,并通过多变量 Cox 回归调整年龄、性别、疾病持续时间、EDSS/SDMT 和 DMT 类别来确定危险比(HR)。
M24 时 GCIPL 变薄 >0.5μm/年对治疗失败预测具有更高的价值(HR:4.5,95%置信区间[CI]:1.8-7.6,p<0.001;特异性 91%,敏感性 81%),其次是 M12 时 GCIPL >0.5μm(优势比[OR]:3.9,95%CI:1.4-6.9,p<0.001;特异性 85%,敏感性 78%)和 M24 时 pRNFL ≥2μm/年(OR:3.7,95%CI:1.1-6.5,p=0.023;特异性 84%,敏感性 69%),而 M12 时的 pRNFL 则没有预测价值。
GCIPL 和 pRNFL 的变薄程度较小,可预测 DMT 起始后残疾进展,可能是 RMS 中治疗失败的有用且可获得的生物标志物。