Bucci Tommaso, Romiti Giulio Francesco, Ishiguchi Hironori, Gerra Luigi, Mantovani Marta, Huang Bi, Proietti Marco, Lip Gregory Y H
Liverpool Centre for Cardiovascular Science at University of Liverpool, Liverpool John Moores University and Liverpool and Heart and Chest Hospital, Liverpool, United Kingdom.
Department of Clinical Internal, Anaesthesiologic and Cardiovascular Sciences, Sapienza University of Rome, Rome, Italy.
EClinicalMedicine. 2024 Dec 1;78:102974. doi: 10.1016/j.eclinm.2024.102974. eCollection 2024 Dec.
Few data are available about the impact of oral anticoagulants (OAC) in patients with Atrial Fibrillation (AF) and clinical complexity (CC).
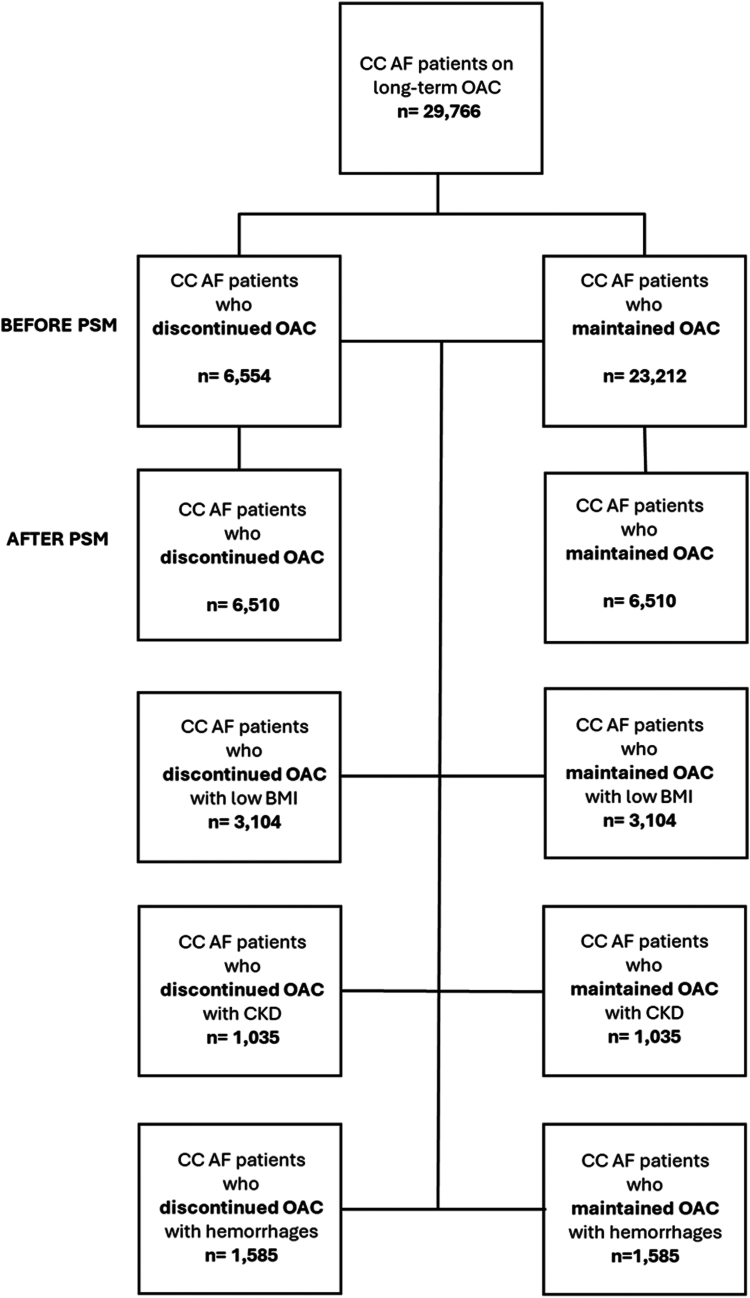
We conducted a retrospective study utilising data from the TriNetX network. Based on ICD-10-CM codes entered between 2020 and 2022, AF patients aged ≥75 years on long-term OAC with CC were categorised into two groups based on OAC use in the year before entering the study (maintained vs discontinued). CC was defined as BMI ≤23 kg/m, and/or history of bleeding, and/or chronic kidney disease. The primary outcomes were the one-year risk of all-cause death, major cardiovascular events (MACE), and major bleeding. Cox regression analyses were used to calculate hazard ratios (HRs) and 95% CIs before and after 1:1 propensity score matching (PSM).
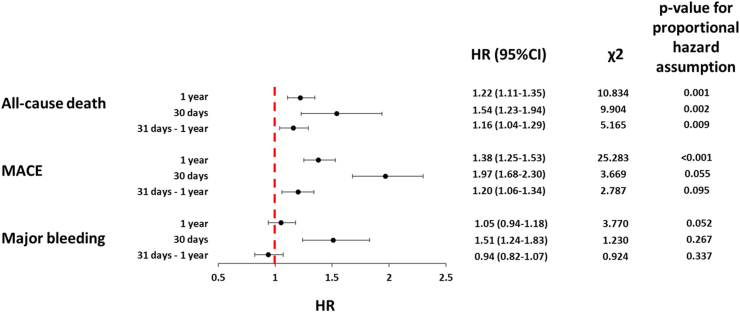
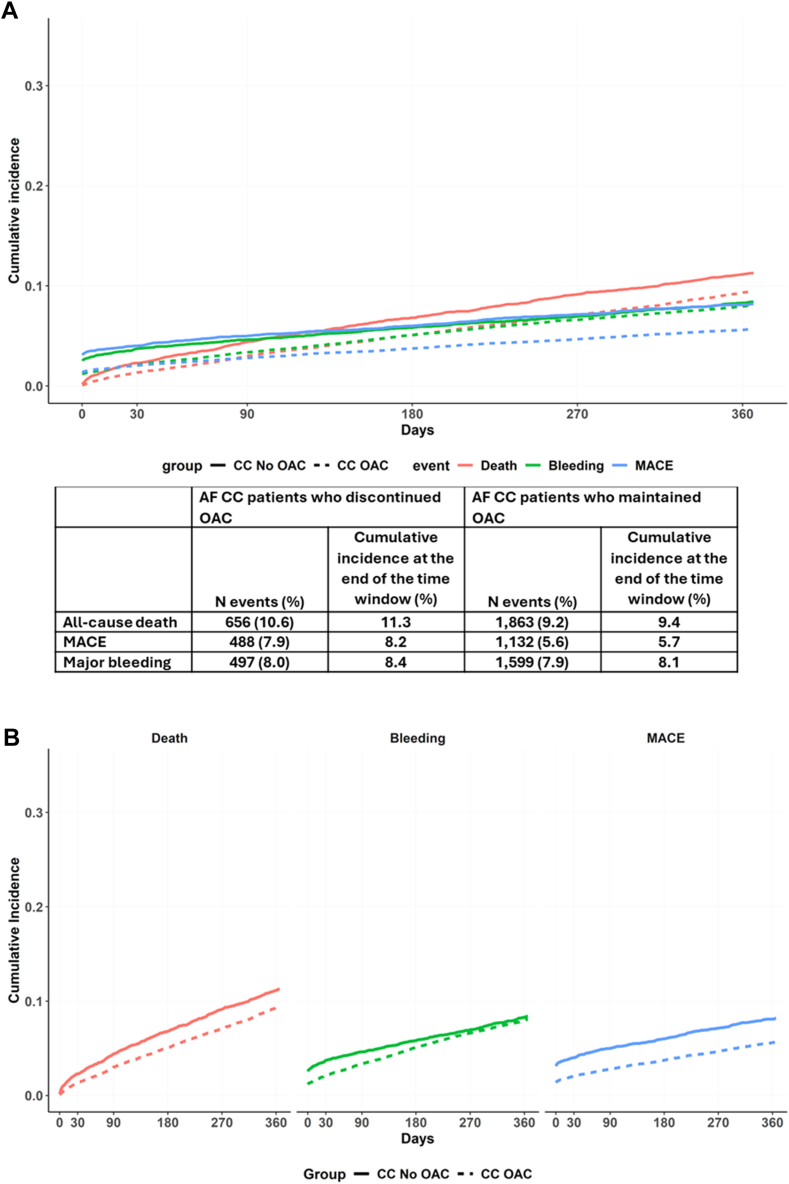
We identified 6554 AF CC patients who discontinued OAC (mean age 81.5 ± 6.0 years, 46.7% females) and 23,212 AF patients with CC who maintained OAC (81.3 ± 6.0 years, 49.4% females). Before PSM, AF CC patients who discontinued OAC had a higher prevalence of intracranial, gastrointestinal haemorrhages, and antiplatelet use, with no significant differences after PSM. OAC discontinuation was associated with a higher risk of all-cause death (HR 1.22, 95% CI 1.11-1.35) and MACE (HR 1.38, 95% CI 1.25-1.53). The one-year risk of major bleeding was similar in those who discontinued or maintained OAC (HR 1.05, 95% CI 0.94-1.18), although it was significantly higher during the early follow-up (HR 1.51, 95% CI 1.24-1.83). The risk of primary outcomes decreased over time, with the risk of bleeding becoming not significant.
AF CC patients who discontinued OAC have a high risk of adverse events. New antithrombotic and integrated care approaches to reduce thrombotic risk without increasing bleeding risk are needed in these patients.
This study received no funding.
关于口服抗凝剂(OAC)对心房颤动(AF)合并临床复杂性(CC)患者的影响,现有数据较少。
我们利用TriNetX网络的数据进行了一项回顾性研究。根据2020年至2022年间录入的国际疾病分类第十版临床修订本(ICD - 10 - CM)编码,将年龄≥75岁、长期服用OAC且合并CC的AF患者,根据进入研究前一年的OAC使用情况(持续使用与停用)分为两组。CC定义为体重指数(BMI)≤23kg/m²,和/或有出血史,和/或患有慢性肾脏病。主要结局为全因死亡、主要心血管事件(MACE)和大出血的一年风险。采用Cox回归分析计算1:1倾向评分匹配(PSM)前后的风险比(HR)和95%置信区间(CI)。
我们识别出6554例停用OAC的AF合并CC患者(平均年龄81.5±6.0岁,46.7%为女性)和23212例持续使用OAC的AF合并CC患者(81.3±6.0岁,49.4%为女性)。在PSM之前,停用OAC的AF合并CC患者颅内、胃肠道出血及使用抗血小板药物的患病率较高,PSM后无显著差异。停用OAC与全因死亡风险较高(HR 1.22,95%CI 1.11 - 1.35)和MACE风险较高(HR 1.38,95%CI 1.25 - 1.53)相关。停用或持续使用OAC的患者大出血的一年风险相似(HR 1.05,95%CI 0.94 - 1.18),尽管在早期随访期间显著更高(HR 1.51,95%CI 1.24 - 1.83)。主要结局的风险随时间降低,出血风险变得不显著。
停用OAC的AF合并CC患者发生不良事件的风险较高。这些患者需要新的抗栓和综合护理方法,以降低血栓形成风险而不增加出血风险。
本研究未获得资金支持。