Bucci Tommaso, Nabradalik Katarzyna, Irlik Krysztof, Shantsila Alena, Romiti Giulio Francesco, Proietti Marco, Teo Wee-Siong, Park Hyung-Wook, Shimizu Wataru, Tse Hung-Fat, Chao Tze-Fan, Lip Gregory Y H
Liverpool Centre for Cardiovascular Science at University of Liverpool, Liverpool John Moores University and Liverpool and Heart and Chest Hospital, Liverpool, United Kingdom.
Department of Clinical Internal, Anesthesiologic and Cardiovascular Sciences, Sapienza University of Rome, Rome, Italy.
Lancet Reg Health West Pac. 2025 May 12;58:101570. doi: 10.1016/j.lanwpc.2025.101570. eCollection 2025 May.
Limited data exist on the effectiveness of the ABC (Atrial Fibrillation Better Care) pathway in reducing adverse events in Asian patients with atrial fibrillation (AF) and chronic kidney disease (CKD).
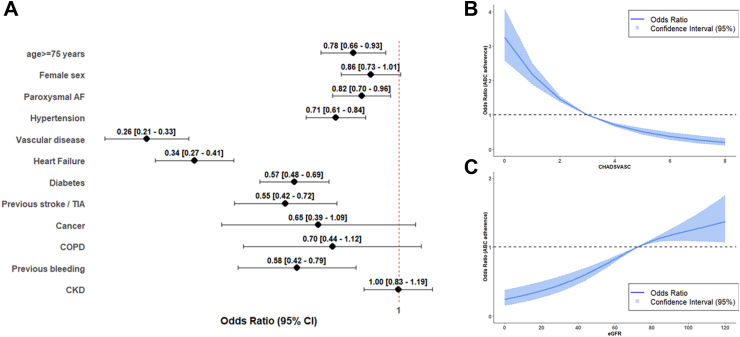
A post-hoc analysis of the prospective APHRS AF Registry. Patients were divided into CKD (eGFR < 60 ml/min) and non-CKD (eGFR ≥ 60 ml/min) groups. Logistic regression assessed factors associated with CKD, oral anticoagulant (OAC) use, and rhythm control strategies. Cox regression estimated hazard ratios (HRs) for a composite outcome of all-cause mortality and major adverse cardiovascular events. Subgroup analyses evaluated outcomes by CKD severity and ABC adherence.
Of 3550 patients, 1029 had CKD (mean age 75.3 ± 10.3 years, 40.3% female), and 2521 did not (66.4 ± 11.3 years, 32.3% female). CKD patients were older, more often female, had lower ABC adherence (29.5% vs. 42.1%, p < 0.001) and anticoagulation use (Odds Ratio [OR] 0.77, 95% CI 0.61-0.96), but higher warfarin use, and were less likely to receive rhythm control (OR 0.79, 95% CI 0.66-0.94) comparing to those without CKD. CKD and adherence to the ABC pathway were independently associated with higher (HR 1.90, 95% CI 1.46-2.48) and lower (HR 0.64, 95% CI 0.48-0.87) risks of the composite outcome, respectively. Adverse event risks increased with CKD severity, and ABC pathway benefits were observed irrespective of CKD.
AF patients with CKD show lower ABC pathway adherence and high risk of adverse events. Improving adherence to integrated care approaches may improve prognosis in this patient group.
This study was an independent research grant by Pfizer and Bristol Myers Squibb (BMS) to APHRS.
关于房颤更好治疗(ABC)路径在降低亚洲房颤(AF)合并慢性肾脏病(CKD)患者不良事件方面的有效性,现有数据有限。
对前瞻性亚太心律学会房颤注册研究进行事后分析。患者被分为CKD组(估算肾小球滤过率[eGFR]<60 ml/分钟)和非CKD组(eGFR≥60 ml/分钟)。逻辑回归评估与CKD、口服抗凝药(OAC)使用及节律控制策略相关的因素。Cox回归估计全因死亡率和主要不良心血管事件复合结局的风险比(HR)。亚组分析按CKD严重程度和ABC路径依从性评估结局。
在3550例患者中,1029例有CKD(平均年龄75.3±10.3岁,40.3%为女性),2521例没有CKD(66.4±11.3岁,32.3%为女性)。CKD患者年龄更大,女性更多见,ABC路径依从性更低(29.5%对42.1%,p<0.001),抗凝药使用更少(优势比[OR]0.77,95%置信区间[CI]0.61 - 0.96),但华法林使用更多,与无CKD患者相比,接受节律控制的可能性更小(OR 0.79,95%CI 0.66 - 0.94)。CKD和ABC路径依从性分别与复合结局的高风险(HR 1.90,95%CI 1.46 - 2.48)和低风险(HR 0.64,95%CI 0.48 - 0.87)独立相关。不良事件风险随CKD严重程度增加,且无论CKD情况如何,均可观察到ABC路径的益处。
AF合并CKD患者ABC路径依从性较低,不良事件风险高。提高对综合治疗方法的依从性可能改善该患者群体的预后。
本研究是辉瑞公司和百时美施贵宝公司(BMS)给予亚太心律学会的独立研究资助。