Nicholson Jill Theresa, Cleary Sinead, Farmer Gemma, Monaghan Orla, O' Driscoll Hannah, Nugent Killian, Khosravi Bahareh, Quinlan Eaine, McArdle Orla, Duane Fran K
St. Luke's Radiation Oncology Network, St. Luke's Hospital, Dublin, Ireland.
Discipline of Radiation Therapy &Trinity St James's Cancer Institute, Trinity College Dublin, Ireland.
Adv Radiat Oncol. 2024 Nov 5;10(1):101668. doi: 10.1016/j.adro.2024.101668. eCollection 2025 Jan.
In March 2020, a 1-week ultrahypofractionated adjuvant breast radiation therapy schedule, 26 Gy in 5 fractions, and telehealth were adopted to reduce the risk of COVID-19 for staff and patients. This study describes real-world 1-year late toxicity for ultrahypofractionation (including a sequential boost) and patient perspectives on this new schedule and telehealth workflows.
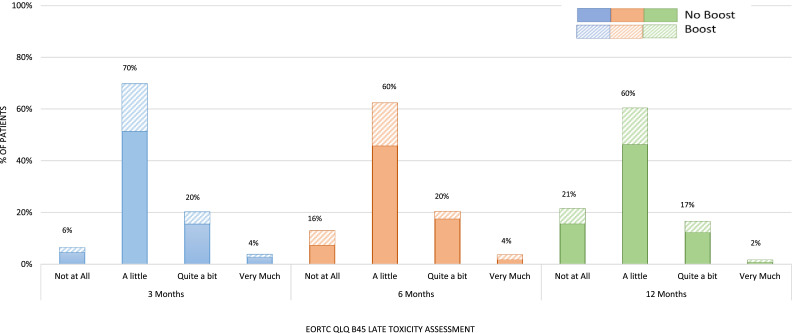
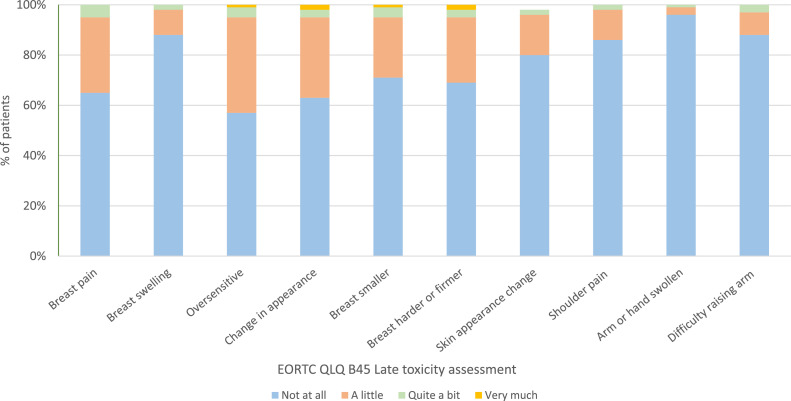
Consecutive patients were enrolled between March and August 2020. Patient-reported outcome measures, including the presence of breast pain, swelling, firmness, and others, were recorded using the European Organisation for research and treatment of cancer quality of life questionairre (EORTC QLQ) BR45 at baseline, 3 months, 6 months, and 1 year. Virtual teleconferencing without video was used. Patients were invited to use video at 1 year for a physician-based assessment, including breast inspection. Patient-reported experience measures were also collected at 1 year to capture how a shortened schedule and telehealth influenced patient experience.
In total, 121 of 135 patients completed at least 2 assessments, of which 33 (25%) received a sequential boost. The majority of patients reported no toxicity or mild toxicity at all 3 time points: 76% at 3 months, 76% at 6 months, and 82% at 1 year. When comparing 26 Gy in 5 fractions alone versus 26 Gy in 5 fractions followed by a sequential boost, there was no difference in toxicity reported at 1 year. A total of 94% felt supported by the medical team throughout their treatment course using telehealth-only consultations. Only 27% actually agreed to video consultation for the purpose of breast inspection when offered.
Ultrahypofractionated breast radiation therapy leads to acceptable late toxicity at 1 year, even when followed by a hypofractionated tumor bed boost. Patient satisfaction with ultrahypofractionated treatment and virtual consultations without video was high. Further investigation concerning the patient's acceptance of video consultations for a physician-based assessment, including breast inspection, is warranted.
2020年3月,采用了为期1周的超分割辅助性乳腺放射治疗方案(5次分割,共26 Gy)以及远程医疗,以降低工作人员和患者感染新冠病毒的风险。本研究描述了超分割放疗(包括序贯推量)的1年现实世界晚期毒性反应,以及患者对这一新方案和远程医疗工作流程的看法。
2020年3月至8月纳入连续的患者。使用欧洲癌症研究与治疗组织生活质量问卷(EORTC QLQ)BR45在基线、3个月、6个月和1年时记录患者报告的结局指标,包括乳房疼痛、肿胀、硬度等情况。采用无视频的虚拟电话会议。邀请患者在1年时使用视频进行基于医生的评估,包括乳房检查。在1年时还收集了患者报告的体验指标,以了解缩短的治疗方案和远程医疗如何影响患者体验。
135例患者中,共有121例完成了至少2次评估,其中33例(25%)接受了序贯推量。大多数患者在所有3个时间点均报告无毒性或轻度毒性:3个月时为76%,6个月时为76%,1年时为82%。比较单纯5次分割26 Gy与5次分割26 Gy后序贯推量,1年时报告的毒性反应无差异。共有94%的患者在整个治疗过程中仅通过远程医疗咨询就感受到了医疗团队的支持。当提供视频咨询用于乳房检查时,只有27%的患者实际同意。
超分割乳腺放射治疗在1年时导致可接受的晚期毒性反应,即使在随后进行低分割瘤床推量时也是如此。患者对超分割治疗和无视频的虚拟咨询满意度较高。有必要进一步调查患者对用于基于医生的评估(包括乳房检查)的视频咨询的接受情况。