Andrianopoulou S, Fiedler L S, Lippert B M, Bulut O C
Department for Otorhinolaryngology, Head and Neck, Plastic Surgery, SLK Clinics, Heilbronn, Baden-Württemberg, Germany.
Medical University Heidelberg, Heidelberg, Baden-Württemberg, Germany.
Int J Surg Oncol. 2024 Dec 9;2024:7598063. doi: 10.1155/ijso/7598063. eCollection 2024.
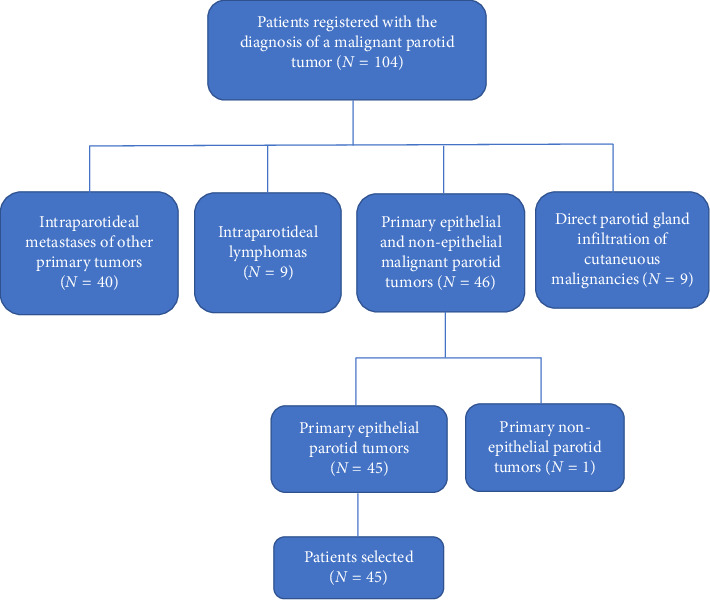
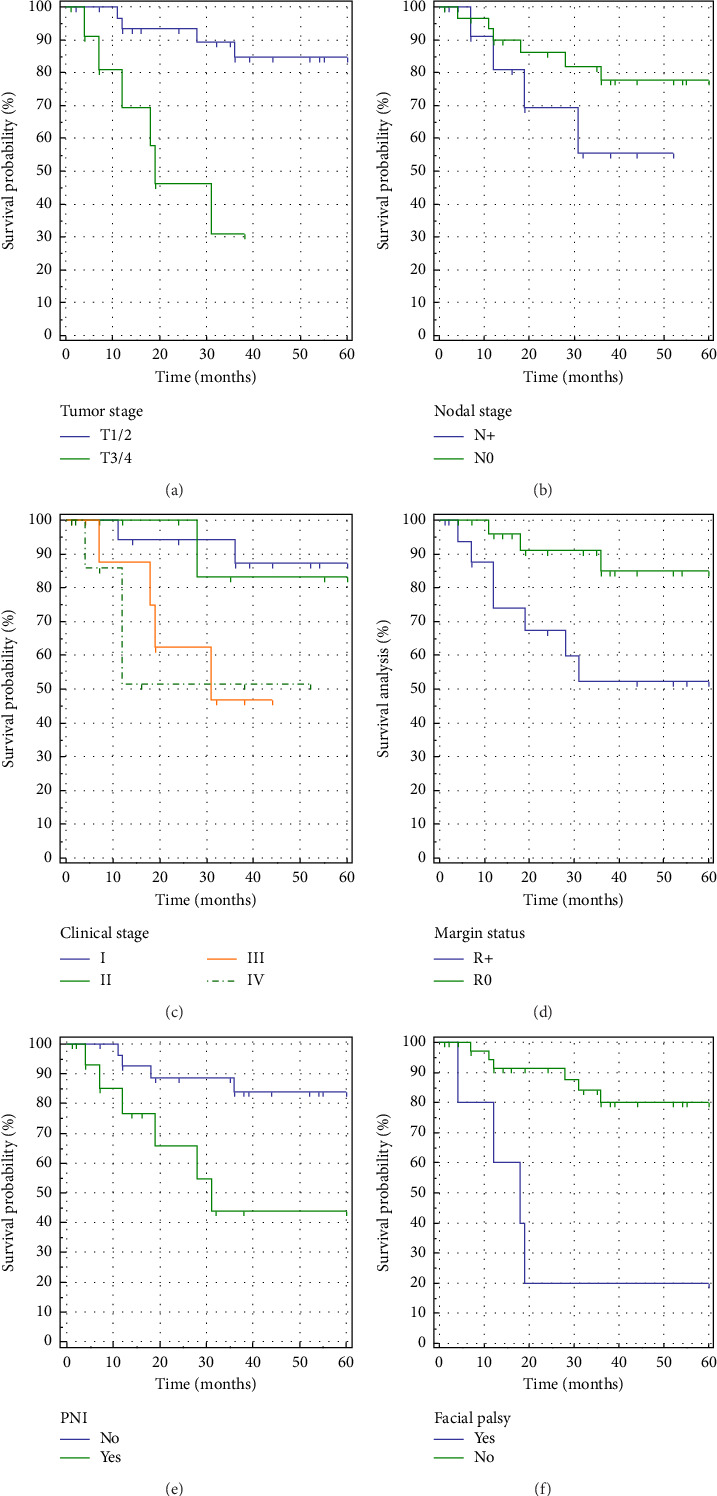
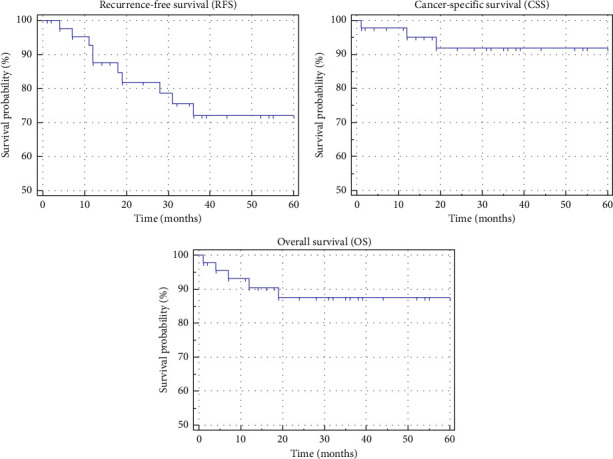
This study sought to comprehensively evaluate the diagnosis, therapeutic interventions, and outcomes of individuals afflicted with malignant parotid tumors at a tertiary care otolaryngology department in Heilbronn, Germany, spanning the years 2010-2018. The primary objective was to juxtapose this dataset with findings from analogous single and multicenter investigations. We conducted a meticulous analysis of electronic medical records pertaining to 45 patients subjected to primary parotid cancer treatment. The male-to-female ratio was 3:2, with an average age of 61 years. Predominant histological types included mucoepidermoid and squamous cell carcinomas, with ultrasound emerging as the predominant diagnostic modality (97.8% sensitivity). Intraoperative frozen sections exhibited a high level of sensitivity. Notably, lymph node metastasis was prevalent in T3 tumors, frequently located intraparotid and at Neck level II. Solely one patient exhibited distant metastases (pulmonary). All patients underwent parotidectomy, and 29% necessitated a secondary procedure due to positive resection margins. Postoperative complications encompassed facial nerve palsy, seromas, and salivary fistulas. Adjuvant radiotherapy (38%) was recommended for high-grade tumors, T3/T4 stage, N+, perineural invasion (PNI), and positive or uncertain surgical margins. Neck dissection was executed in 67% of instances, with 20% revealing occult lymph node metastases. Recurrence manifested in 22% of patients, primarily as locoregional recurrence (80%) and distant metastases (20%). The 3-year recurrence-free survival (RFS), cancer-specific survival (CSS), and overall survival (OS) rates stood at 72.1%, 91.9%, and 87.5%, respectively. Noteworthy factors influencing RFS included preoperative facial palsy, T stage, resection margins, and PNI. In summary, the management of parotid cancer involving surgical interventions, neck dissection, and radiotherapy in high-risk patients yielded commendable outcomes with minimal complications, showcasing survival rates exceeding 70%. Timely diagnosis at an early stage is imperative for achieving tumor-free margins and enhancing survival rates. More assertive therapeutic strategies are advocated for cases presenting with preoperative facial nerve palsy and PNI.
本研究旨在全面评估2010年至2018年期间德国海尔布隆一家三级护理耳鼻喉科中患有腮腺恶性肿瘤患者的诊断、治疗干预措施及治疗结果。主要目的是将该数据集与类似的单中心和多中心研究结果进行对比。我们对45例接受原发性腮腺癌治疗患者的电子病历进行了细致分析。男女比例为3:2,平均年龄为61岁。主要组织学类型包括黏液表皮样癌和鳞状细胞癌,超声是主要的诊断方式(敏感性为97.8%)。术中冰冻切片显示出较高的敏感性。值得注意的是,T3期肿瘤中淋巴结转移较为常见,常位于腮腺内和颈部II区。仅1例患者出现远处转移(肺部)。所有患者均接受了腮腺切除术,29%的患者因手术切缘阳性而需要二次手术。术后并发症包括面神经麻痹、血清肿和涎瘘。对于高级别肿瘤、T3/T4期、N+、神经周围浸润(PNI)以及手术切缘阳性或不确定的患者,建议进行辅助放疗(38%)。67%的病例进行了颈部清扫,其中20%发现隐匿性淋巴结转移。22%的患者出现复发,主要为局部区域复发(80%)和远处转移(20%)。3年无复发生存率(RFS)、癌症特异性生存率(CSS)和总生存率(OS)分别为72.1%、91.9%和87.5%。影响RFS的显著因素包括术前面神经麻痹、T分期、手术切缘和PNI。总之,对腮腺癌患者进行手术干预、颈部清扫以及对高危患者进行放疗,并发症极少,取得了值得称赞的结果,生存率超过70%。早期及时诊断对于实现无瘤切缘和提高生存率至关重要。对于术前出现面神经麻痹和PNI的病例,提倡采取更积极的治疗策略。