Lehman Alice, Tessier Katelyn M, Sattarova Victoria, Montezuma Sandra Rocio, Kline Susan, Erayil Serin Edwin
Division of Infectious Diseases and International Medicine, University of Minnesota, Minneapolis, Minnesota, USA.
Masonic Cancer Center, Biostatistics Core, University of Minnesota, Minneapolis, Minnesota, USA.
Open Forum Infect Dis. 2024 Nov 7;11(12):ofae663. doi: 10.1093/ofid/ofae663. eCollection 2024 Dec.
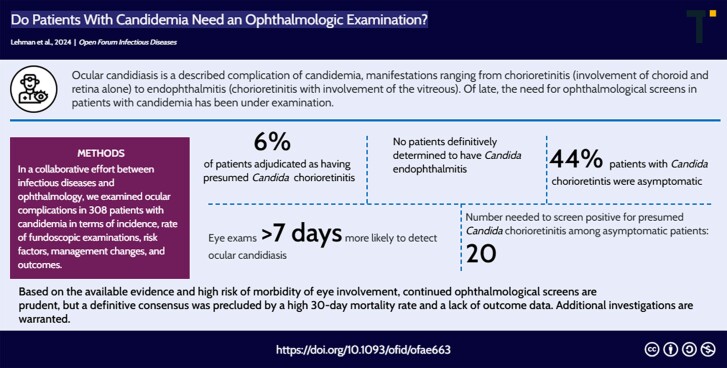
The Infectious Diseases Society of America recommends a screening dilated retinal examination by an ophthalmologist for all patients with candidemia. Conversely, the American Academy of Ophthalmology recommends against routine screening in patients with candidemia without symptoms.
In a collaborative effort between infectious diseases and ophthalmology, we examined the incidence of ocular complications in 308 patients with candidemia and subsequently measured the rate of fundoscopic examinations, risk factors for ocular complications, management changes, and outcomes.
Among those who received fundoscopic exams, findings suspicious for ocular candidiasis were found in 12 patients (8%, 12/148). After independent review by ophthalmology and infectious diseases, 3 patients were found to have alternate pathologies that explained their ocular findings. Nine patients (6%, 9/148) were adjudicated as having presumed chorioretinitis. Of these 9 patients, 4 (44%) were asymptomatic, and 2 (22%) were unable to declare symptoms. No patients were definitively determined to have endophthalmitis. Ocular candidiasis was not found to have a statistically significant association with symptoms or comorbidities. Ocular candidiasis was more likely to be found at ophthalmology exams >7 days from first positive blood culture. The number needed to screen to detect presumed chorioretinitis among asymptomatic patients was 20.
Based on the available evidence and high risk of morbidity of eye involvement, continued ophthalmological screens seem prudent, but a definitive consensus was found to be challenging given a lack of outcome data. Additional investigations are warranted. Ophthalmology screenings have a higher sensitivity at >7 days from positive blood culture.
美国传染病学会建议,对所有念珠菌血症患者均应由眼科医生进行散瞳视网膜检查。相反,美国眼科学会不建议对无症状的念珠菌血症患者进行常规筛查。
通过传染病科与眼科的合作,我们检查了308例念珠菌血症患者的眼部并发症发生率,随后测量了眼底检查率、眼部并发症的危险因素、管理变化及结果。
在接受眼底检查的患者中,12例(8%,12/148)发现有可疑的眼部念珠菌病表现。经眼科和传染病科独立评估后,发现3例患者有其他病变可以解释其眼部表现。9例(6%,9/148)被判定为疑似脉络膜视网膜炎。在这9例患者中,4例(44%)无症状,2例(22%)无法表述症状。没有患者被明确诊断为眼内炎。未发现眼部念珠菌病与症状或合并症之间存在统计学上的显著关联。在首次血培养阳性7天以上接受眼科检查的患者中,更有可能发现眼部念珠菌病。在无症状患者中,筛查出疑似脉络膜视网膜炎所需的例数为20例。
基于现有证据以及眼部受累的高发病风险,继续进行眼科筛查似乎是谨慎的做法,但鉴于缺乏结局数据,很难达成明确的共识。有必要进行更多研究。在血培养阳性7天以上进行眼科筛查具有更高的敏感性。