Oliva A, Volpicelli L, Gigante A, Di Nillo M, Trapani S, Viscido A, Sacco F, Mastroianni C M
Department of Public Health and Infectious Diseases, Sapienza University of Rome, Piazzale Aldo Moro 5, Rome 00185, Italy.
Department of Translational and Precision Medicine, Sapienza University of Rome, Viale dell'Università 37, Rome 00185, Italy.
JAC Antimicrob Resist. 2024 Dec 17;6(6):dlae201. doi: 10.1093/jacamr/dlae201. eCollection 2024 Dec.
Bloodstream infections (BSIs) caused by KPC-producing (KPC-Kp) are still associated with high mortality, and the game-changing drug ceftazidime/avibactam has shown suboptimal pharmacokinetics in some clinical settings. Ceftazidime/avibactam renal dose adjustment has recently been identified as an independent risk factor for mortality.
To investigate the effect of ceftazidime/avibactam renal dose adjustment on mortality.
Patients with KPC-Kp BSI treated with a ceftazidime/avibactam-based regimen were retrospectively collected and analysed. The primary outcome was mortality at 7, 14 and 30 days after the start of definitive ceftazidime/avibactam antibiotic therapy. Renal function was estimated using the CKD-EPI equation.
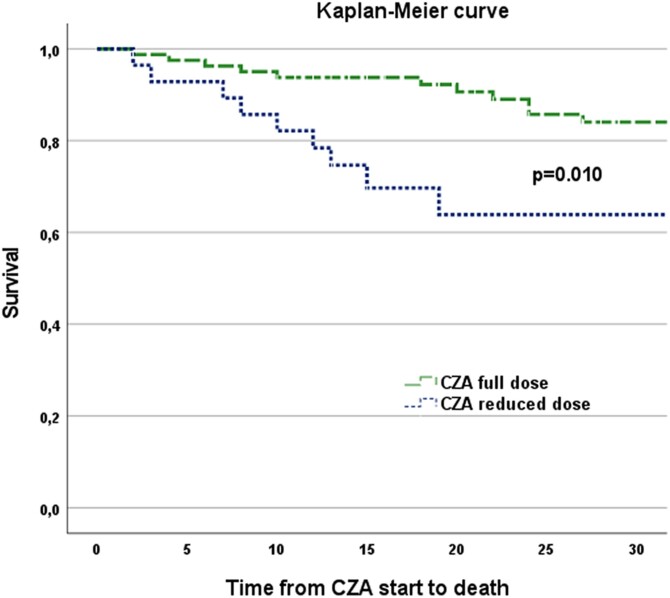
One hundred and ten patients with KPC-Kp BSI treated with a ceftazidime/avibactam-based regimen were included. Full-dose ceftazidime/avibactam (7.5 g daily) was prescribed to 82 patients (74.5%), while 28 patients (25.5%) received a renal-adjusted dose (17 patients due to chronic renal disease or haemodialysis, 11 patients due to infection-related acute kidney injury), with a median of 1.9 g daily. At multivariable analysis, receiving a reduced dose of ceftazidime/avibactam was independently associated with mortality (HR 4.47, 95% CI 1.09-18.03, = 0.037), along with intra-abdominal or lower respiratory tract infections as source of BSI (HR 5.42, 95% CI 1.77-16.55, = 0.003), septic shock (HR 6.99, 95% CI 1.36-35.87, = 0.020) and SARS-CoV-2 coinfection (HR 10.23, 95% CI 2.69-38.85, = 0.001).
Dose reduction of ceftazidime/avibactam according to renal function in patients with KPC-Kp BSI seems to be independently associated with higher mortality. This may be possibly due to inadequate exposure provided by the recommended doses for renal impairment.
产KPC酶的肺炎克雷伯菌(KPC-Kp)引起的血流感染(BSIs)仍与高死亡率相关,而具有变革性的药物头孢他啶/阿维巴坦在某些临床环境中显示出不理想的药代动力学。最近已确定头孢他啶/阿维巴坦的肾脏剂量调整是死亡率的独立危险因素。
研究头孢他啶/阿维巴坦肾脏剂量调整对死亡率的影响。
回顾性收集并分析接受以头孢他啶/阿维巴坦为基础方案治疗的KPC-Kp BSI患者。主要结局是在确定的头孢他啶/阿维巴坦抗生素治疗开始后7、14和30天的死亡率。使用CKD-EPI方程估算肾功能。
纳入110例接受以头孢他啶/阿维巴坦为基础方案治疗的KPC-Kp BSI患者。82例患者(74.5%)接受全剂量头孢他啶/阿维巴坦(每日7.5 g),而28例患者(25.5%)接受肾脏调整剂量(17例因慢性肾病或血液透析,11例因感染相关急性肾损伤),中位数为每日1.9 g。在多变量分析中,接受降低剂量的头孢他啶/阿维巴坦与死亡率独立相关(HR 4.47,95%CI 1.09-18.03,P = 0.037),同时腹腔内或下呼吸道感染作为BSI的来源(HR 5.42,95%CI 1.77-16.55,P = 0.003)、感染性休克(HR 6.99,95%CI 1.36-35.87,P = 0.020)和SARS-CoV-2合并感染(HR 10.23,95%CI 2.69-38.85,P = 0.001)。
KPC-Kp BSI患者根据肾功能降低头孢他啶/阿维巴坦剂量似乎与较高死亡率独立相关。这可能是由于针对肾功能损害的推荐剂量提供的暴露不足。