Tubert Perrine, Kalimouttou Alexandre, Bouzat Pierre, David Jean-Stéphane, Gauss Tobias
Department of Anesthesia and Intensive Care, Grenoble-Alpes University Hospital, Grenoble, France.
Inserm, U1216, CHU Grenoble Alpes, Grenoble Institute Neurosciences, Univ. Grenoble Alpes, 38000, Grenoble, France.
Crit Care. 2024 Dec 18;28(1):416. doi: 10.1186/s13054-024-05185-7.
Crystalloid-based fluid resuscitation has long been a cornerstone in the initial management of trauma-induced hemorrhagic shock. However, its benefit is increasingly questioned as it is suspected to increase bleeding and worsen coagulopathy. The emergence of alternative strategies like permissive hypotension and vasopressor use lead to a shift in early trauma care practices. Critical appraisal of current evidence is necessary to guide clinicians and outline research perspectives.
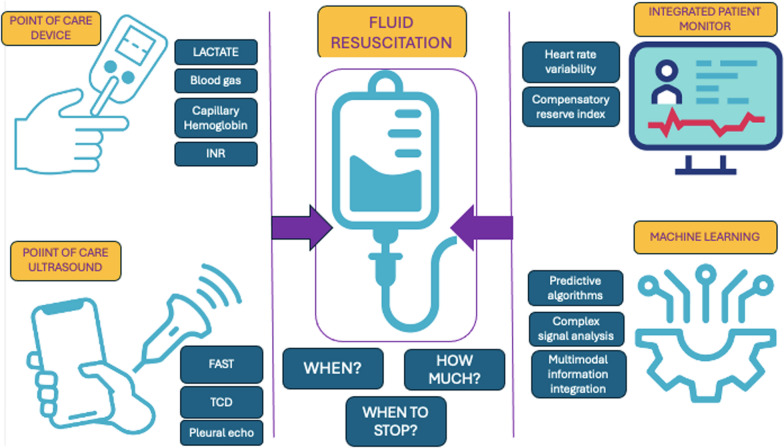
Current guidelines for managing trauma-induced hemorrhagic shock suggest titrating fluids and using vasopressors to achieve minimal blood pressure targets until hemorrhage is controlled. In case of traumatic brain injury with severe hemorrhage, blood pressure target increases. The scientific literature supporting these recommendations is limited, and several aspects remain the subject of ongoing scientific debate. The aim of this review is to evaluate the existing evidence on low-volume fluid resuscitation during the first hours of trauma management, with an emphasis on its integration with permissive hypotension, vasopressor use and cerebral perfusion pressure in traumatic brain injury. The review also highlights the limitations of current guidelines, particularly the lack of robust evidence supporting specific type of fluid, volumes and administration protocols tailored to specific trauma scenarios and populations. Emerging technologies such as point-of-care diagnostics, integrated monitoring systems, and machine learning hold promise for enhancing clinical decision-making in trauma care. These innovations could play a crucial role, ultimately helping clinicians address critical unanswered questions in trauma management and improve patient survival.
Crystalloid-based resuscitation remains relevant in early trauma care, but its application must be reassessed considering recent evidence and evolving practices. Further research is essential to refine fluid resuscitation guidelines, particularly in defining safe fluid volumes and the role of vasopressors. The integration of advanced monitoring technologies may offer new opportunities to optimize trauma care and improve outcomes.
基于晶体液的液体复苏长期以来一直是创伤性失血性休克初始治疗的基石。然而,由于怀疑其会增加出血并加重凝血病,其益处越来越受到质疑。允许性低血压和使用血管升压药等替代策略的出现导致了早期创伤治疗实践的转变。对当前证据进行批判性评估对于指导临床医生并概述研究前景很有必要。
当前创伤性失血性休克管理指南建议滴定液体并使用血管升压药以达到最低血压目标,直至出血得到控制。在伴有严重出血的创伤性脑损伤病例中,血压目标会提高。支持这些建议的科学文献有限,几个方面仍在进行科学辩论。本综述的目的是评估创伤管理最初几小时内小容量液体复苏的现有证据,重点是其与允许性低血压、血管升压药的使用以及创伤性脑损伤中脑灌注压的整合。该综述还强调了当前指南的局限性,特别是缺乏有力证据支持针对特定创伤场景和人群量身定制的特定类型液体、容量和给药方案。即时诊断、综合监测系统和机器学习等新兴技术有望加强创伤护理中的临床决策。这些创新可能发挥关键作用,最终帮助临床医生解决创伤管理中关键的未解决问题并提高患者生存率。
基于晶体液的复苏在早期创伤护理中仍然具有相关性,但必须根据最新证据和不断发展的实践重新评估其应用。进一步的研究对于完善液体复苏指南至关重要,特别是在确定安全的液体容量和血管升压药的作用方面。先进监测技术的整合可能为优化创伤护理和改善治疗结果提供新机会。