Kruit Heidi, Rahkonen Leena
Department of Obstetrics and Gynecology, Helsinki University Hospital and University of Helsinki, Helsinki, Finland.
Acta Obstet Gynecol Scand. 2025 Feb;104(2):400-407. doi: 10.1111/aogs.15036. Epub 2024 Dec 19.
Pre-labor rupture of membranes (PROM) occurs in about 8% of term pregnancies with over 70% delivering spontaneously within 24 h. However, prolonged PROM increases the risk of chorioamnionitis and neonatal sepsis. While misoprostol and oxytocin are considered safe and effective methods of labor induction, most guidelines do not encourage balloon catheter (BC) use following PROM given concerns about increased risk of chorioamnionitis. However, lack of robust evidence exists. This study aimed to compare BC and low-dose oral misoprostol (OM) regarding infectious morbidity and assess the impact of routine antibiotic prophylaxis during BC use on infection prevention.
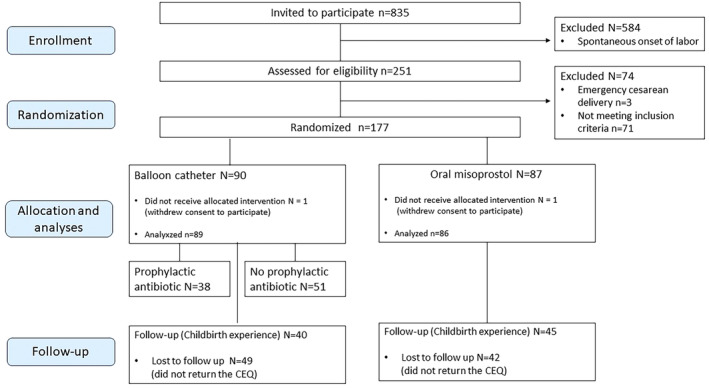
A randomized controlled trial comparing BC and low-dose 25 μg OM for pre-induction cervical ripening in an inpatient setting and assessing the preventive effect of prophylactic antibiotics during BC use in 175 women with PROM was carried out between 1.2.2021 and 31.12.2023 in Helsinki University Hospital. The study protocol was registered in the ISCTN registry (ISRCTN10972090). The primary outcome measures of the study were the mode of delivery, and maternal and neonatal infections.
Eighty-nine women (50.9%) were allocated in the BC arm and 86 women (49.1%) in the OM arm. The cesarean delivery rates were comparable (BC 19.1% [n = 17] vs. OM 11.6% [n = 10]; p = 0.17). The rate of chorioamnionitis (BC 9.1% [n = 8] vs. OM 3.5% [n = 3]; p = 0.21) or neonatal infection (BC 4.5% [n = 4] vs. OM 2.3% [n = 2]; p = 0.68) were not statistically significantly different between the groups, although there was a trend towards higher frequency of infections in the BC arm. There were no differences in the incidence of chorioamnionitis or neonatal infections when routine antibiotic prophylaxis was administered during the BC use compared to those who did not receive antibiotics (chorioamnionitis 10.9% with antibiotics vs. 8.0% without antibiotics; p = 0.68, and neonatal infection 5.3% vs. 3.9%; p = 1.00). Maternal childbirth satisfaction was similar in the BC and OM groups.
Our results showed almost threefold frequency of chorioamnionitis and twofold frequency of neonatal infections following the use of BC compared to OM, although the study was underpowered for reaching statistical significance. The use of prophylactic antibiotics during BC retention did not reduce the incidence of infections.
足月前胎膜早破(PROM)发生于约8%的足月妊娠,其中超过70%的孕妇会在24小时内自然分娩。然而,胎膜早破时间延长会增加绒毛膜羊膜炎和新生儿败血症的风险。虽然米索前列醇和缩宫素被认为是安全有效的引产方法,但由于担心绒毛膜羊膜炎风险增加,大多数指南不鼓励在胎膜早破后使用球囊导管(BC)。然而,目前缺乏有力证据。本研究旨在比较球囊导管和低剂量口服米索前列醇(OM)在感染性发病率方面的差异,并评估在使用球囊导管期间进行常规抗生素预防对预防感染的影响。
2021年2月1日至2023年12月31日期间,在赫尔辛基大学医院对175例胎膜早破孕妇进行了一项随机对照试验,比较球囊导管和低剂量25μg米索前列醇用于引产术前宫颈成熟的效果,并评估在使用球囊导管期间预防性使用抗生素的预防效果。该研究方案已在ISCTN注册中心(ISRCTN10972090)注册。该研究的主要结局指标为分娩方式、孕产妇和新生儿感染情况。
89名女性(50.9%)被分配到球囊导管组,86名女性(49.1%)被分配到米索前列醇组。剖宫产率相当(球囊导管组19.1% [n = 17] vs. 米索前列醇组11.6% [n = 10];p = 0.17)。绒毛膜羊膜炎发生率(球囊导管组9.1% [n = 8] vs. 米索前列醇组3.5% [n = 3];p = 0.21)或新生儿感染率(球囊导管组4.5% [n = 4] vs. 米索前列醇组2.3% [n = 2];p = 0.68)在两组之间无统计学显著差异,尽管球囊导管组的感染频率有升高趋势。与未接受抗生素治疗的患者相比,在使用球囊导管期间进行常规抗生素预防时,绒毛膜羊膜炎或新生儿感染的发生率没有差异(使用抗生素时绒毛膜羊膜炎发生率为10.9%,未使用抗生素时为8.0%;p = 0.68,新生儿感染率分别为5.3%和3.9%;p = 1.00)。球囊导管组和米索前列醇组的产妇分娩满意度相似。
我们的结果显示,与米索前列醇相比,使用球囊导管后绒毛膜羊膜炎的发生率几乎高出两倍,新生儿感染率高出一倍,尽管该研究的样本量不足以达到统计学显著性。在保留球囊导管期间使用预防性抗生素并未降低感染发生率。