Mou Fan, Huang Zhiwei, Cheng Yu, Zhao Xue, Sun Xiujia, Li Huafang, Yu Shunying
Genetics and Biochemistry Laboratory, Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine, Shanghai, China.
Drug Clinical Trial Institution, Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine, Shanghai, China.
Ther Adv Drug Saf. 2024 Dec 18;15:20420986241303432. doi: 10.1177/20420986241303432. eCollection 2024.
Aripiprazole and risperidone, widely used atypical antipsychotics, are commonly adjunctively prescribed in clinical practice. When aripiprazole was combined with risperidone, the genotype of drug-metabolizing enzymes and liver impairment may lead to complex pharmacokinetic changes. The Physiologically Based Pharmacokinetic (PBPK) model can predict the influence of these factors on plasma concentration and optimize dosage regimens.
This study aims to investigate the pharmacokinetic changes of aripiprazole caused by various influencing factors when it was co-administered with risperidone through PBPK models.
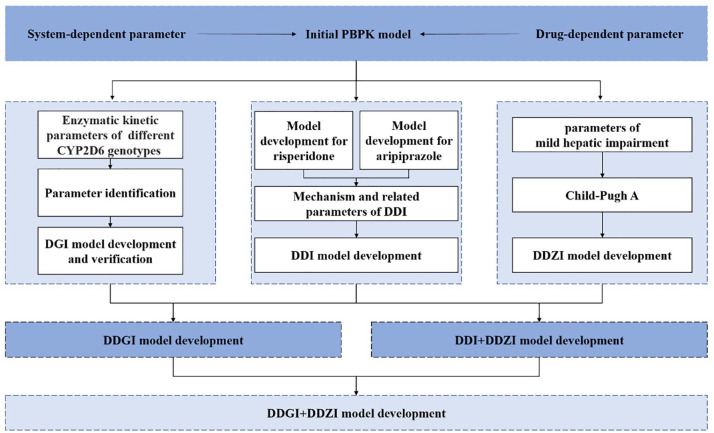
The PBPK models of aripiprazole and risperidone were developed by gathering physicochemical parameters and drug-specific parameters. Then, by combining the inhibitory parameters, the enzymatic kinetic parameters of CYP2D6 genotypes, and the changes in anatomical and physiological parameters when liver function is damaged, the corresponding PBPK models were further established. Finally, this study put forward dosage optimization recommendations for situations where risks may exist.
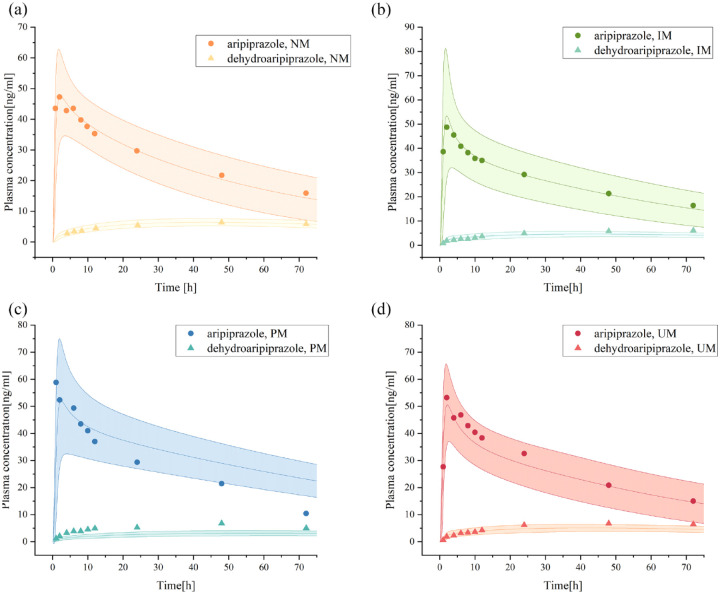
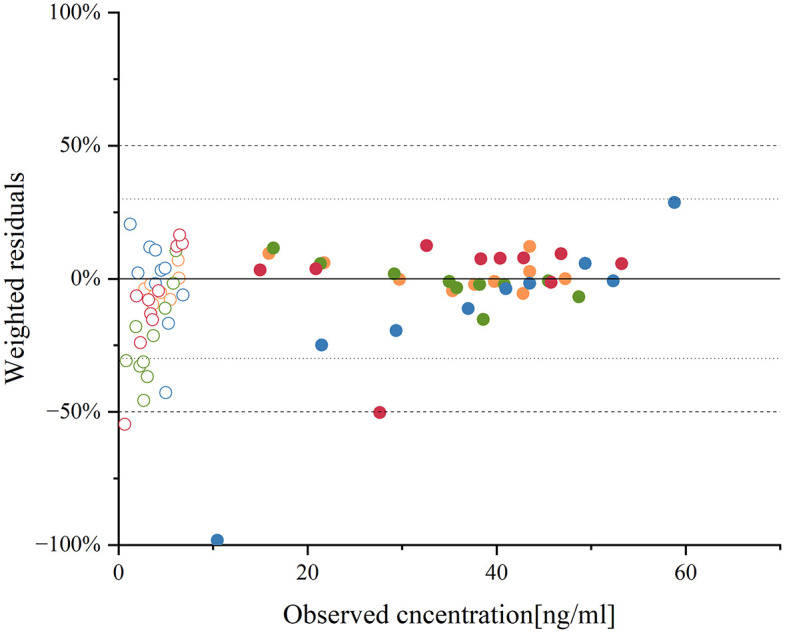
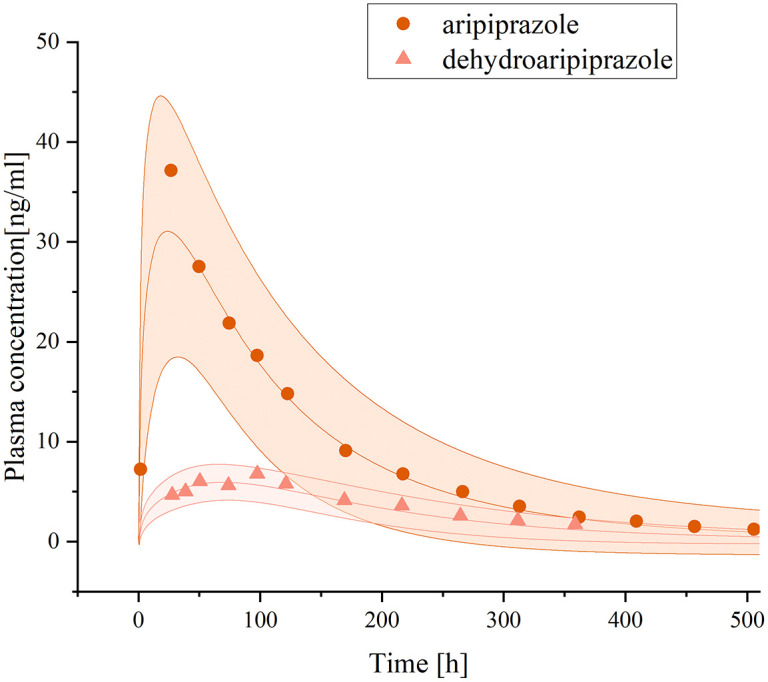
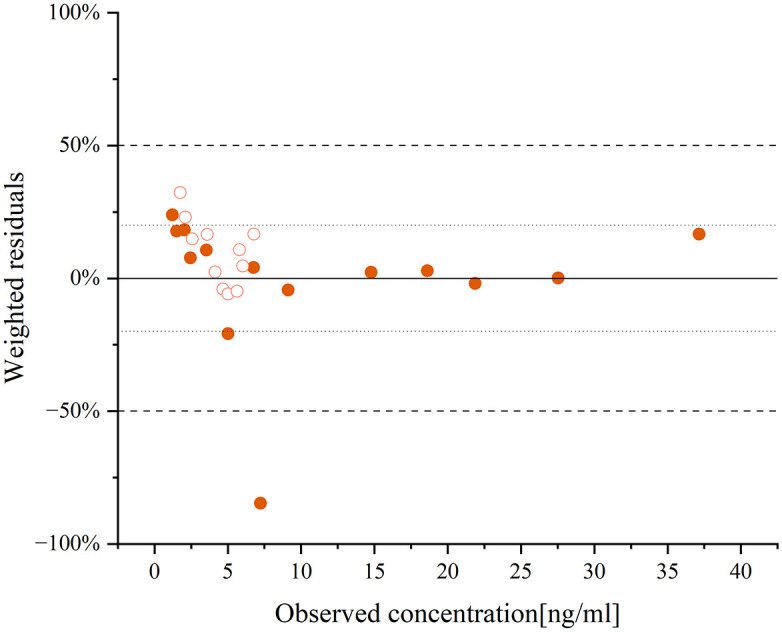
The comparison between predicted and observed plasma concentration data, along with the assessment of pharmacokinetic parameters, was utilized to evaluate the fit performance of the models.
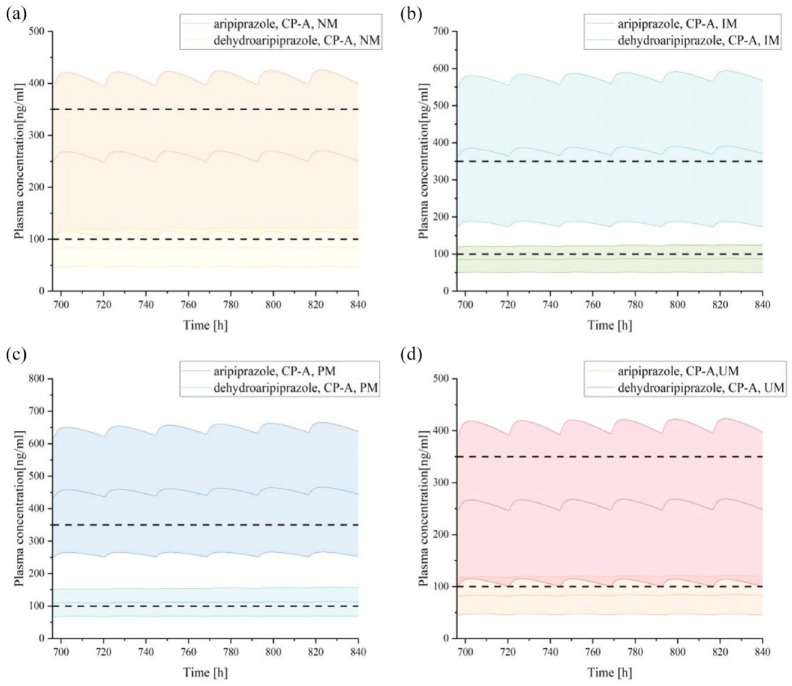
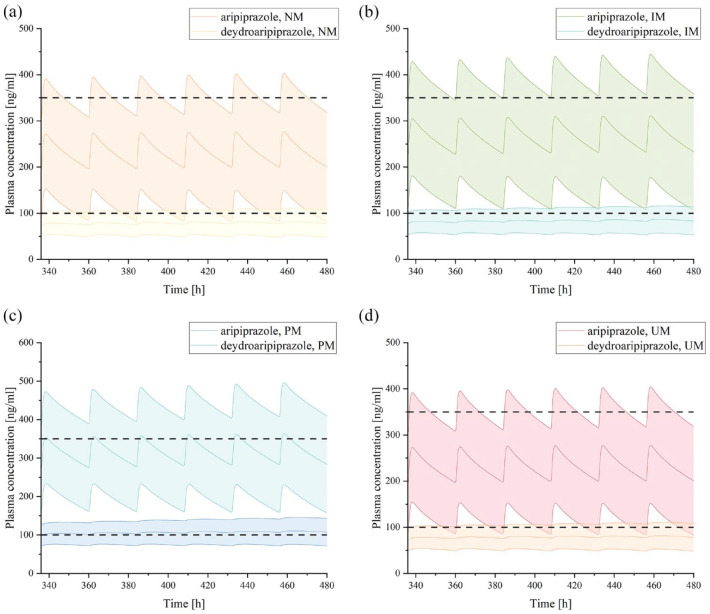
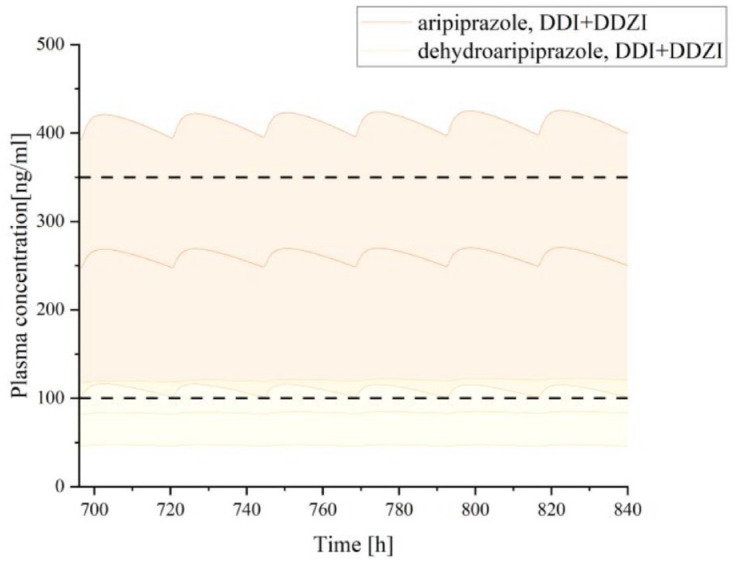
The simulations of the PBPK model revealed that co-administration of risperidone did not result in significant changes in aripiprazole pharmacokinetics. However, in individuals with mild hepatic impairment and CYP2D6 normal metabolizer, a dose reduction of approximately 11% was advised when aripiprazole was combined with risperidone. When individuals with mild liver damage have CYP2D6 genotypes of intermediate metabolizer (IM) and poor metabolizer (PM), aripiprazole doses should be further reduced to 61% and 51%, respectively.
The co-administration of aripiprazole and risperidone is generally considered safe from a pharmacokinetic perspective. However, if individuals have a CYP2D6 genotype of IM or PM and/or if they have mild hepatic impairment, adjusting the dose of aripiprazole is advisable to mitigate potential risks when combining it with risperidone.
阿立哌唑和利培酮是广泛使用的非典型抗精神病药物,在临床实践中常联合使用。当阿立哌唑与利培酮合用时,药物代谢酶的基因型和肝功能损害可能导致复杂的药代动力学变化。基于生理的药代动力学(PBPK)模型可以预测这些因素对血浆浓度的影响并优化给药方案。
本研究旨在通过PBPK模型研究阿立哌唑与利培酮合用时各种影响因素引起的药代动力学变化。
通过收集理化参数和药物特异性参数建立阿立哌唑和利培酮的PBPK模型。然后,结合抑制参数、CYP2D6基因型的酶动力学参数以及肝功能受损时解剖和生理参数的变化,进一步建立相应的PBPK模型。最后,本研究针对可能存在风险的情况提出了剂量优化建议。
利用预测血浆浓度数据与实测数据的比较以及药代动力学参数评估来评价模型的拟合性能。
PBPK模型模拟显示,利培酮与阿立哌唑合用时,阿立哌唑的药代动力学无显著变化。然而,在轻度肝功能损害且CYP2D6为正常代谢型的个体中,阿立哌唑与利培酮合用时建议剂量降低约11%。当轻度肝损伤个体的CYP2D6基因型为中间代谢型(IM)和慢代谢型(PM)时,阿立哌唑剂量应分别进一步降低至61%和51%。
从药代动力学角度来看,阿立哌唑与利培酮联合使用一般被认为是安全的。然而,如果个体具有IM或PM的CYP2D6基因型和/或存在轻度肝功能损害,在将阿立哌唑与利培酮联合使用时,建议调整阿立哌唑剂量以降低潜在风险。